Li Xin, Wang Junpeng, Yao Yun, Yang Lei, Li Zhiqin, Yu Cheng, Zhao Peiyan, Yu Yongli, Wang Liying
Department of Molecular Biology, College of Basic Medical Sciences, Norman Bethune Health Science Center, Jilin University, Changchun 130021, China.
Department of Urology, Henan Provincial People's Hospital, Zhengzhou 450003, China.
Oncotarget. 2017 Jul 1;8(48):83637-83649. doi: 10.18632/oncotarget.18906. eCollection 2017 Oct 13.
We aimed to compare and rank the effects of 9 immune checkpoint inhibitor-related therapies for treating advanced melanoma.
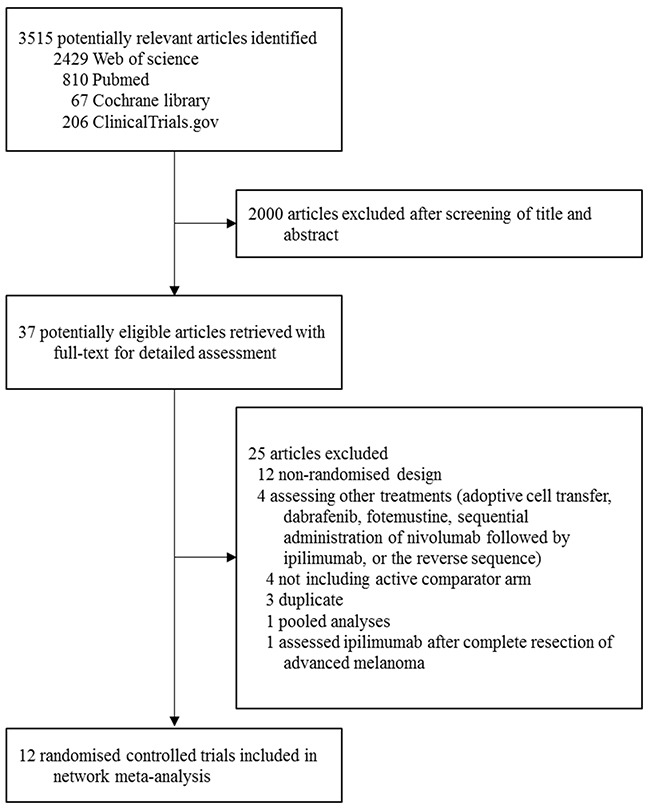
We searched Pubmed, Cochrane databases, Web of Science, and ClinicalTrials.gov for randomized controlled trials of the immune checkpoint inhibitor-related treatments for advanced melanoma. Analysis was done on a Bayesian framework.
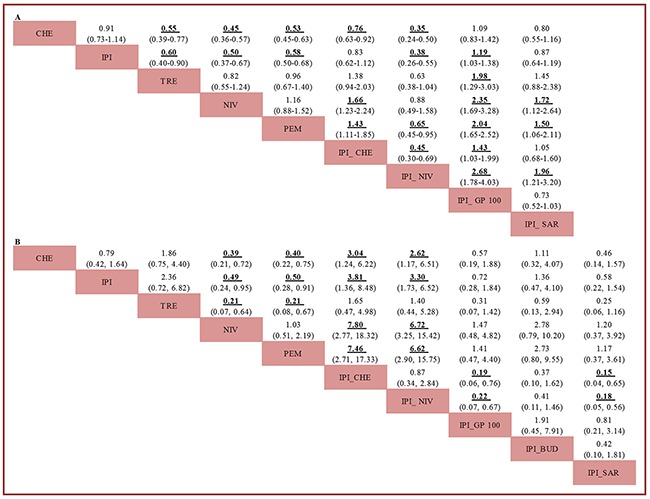
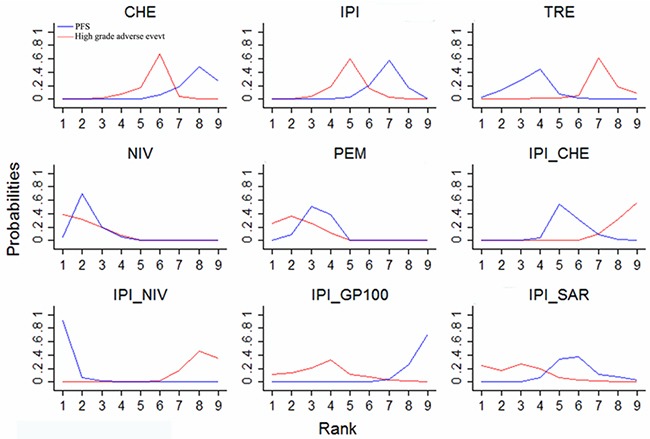
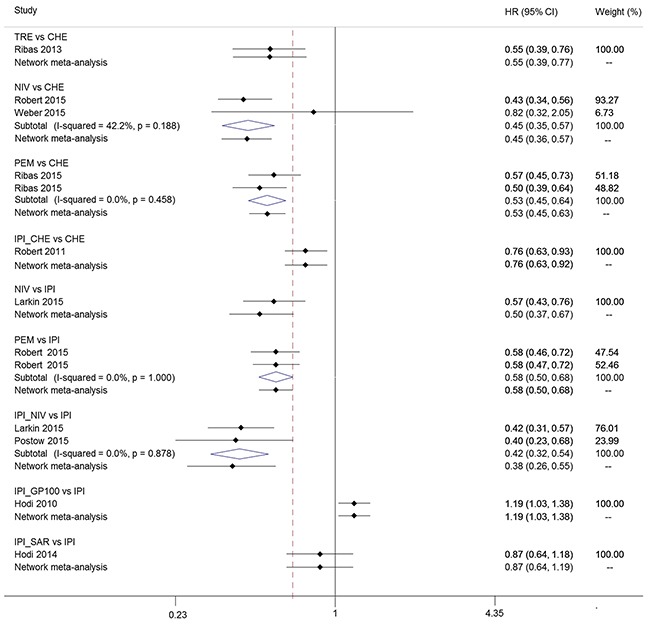
Twelve trials including 5413 patients were identified. Ipilimumab plus nivolumab, nivolumab, and pembrolizumab were significantly more efficacious for progression-free survival (PFS) than ipilimumab (hazard ratio [HR], 0.38, 0.50, and 0.58, respectively), ipilimumab plus chemotherapy (0.45, 0.60, and 0.70, respectively), or ipilimumab plus sargramostim (0.44, 0.57, and 0.67, respectively). Ipilimumab plus gp100 was significantly less efficacious for PFS than the remaining eight immune checkpoint inhibitor-related strategies. Pembrolizumab was significantly more efficacious than ipilimumab and ipilimumab plus gp100 (HR, 0.66, and 0.64, respectively) in improving overall survival (OS). Nivolumab significantly improved OS over tremelimumab (HR, 0.48). Ipilimumab plus sargramostim was ranked the second most effective strategy in terms of OS and well tolerated. Nivolumab and pembrolizumab showed the best profile of acceptability, with significantly less high-grade adverse events than ipilimumab (odds ratio [OR], 0.49 and 0.50, respectively), tremelimumab (0.21 and 0.21, respectively), ipilimumab plus chemotherapy (0.13 and 0.13, respectively), or ipilimumab plus nivolumab (0.15 and 0.15, respectively).
Nivolumab, pembrolizumab and ipilimumab plus sargramostim might be optimum treatments for advanced melanoma because they have the most favorable balance between benefits and acceptability. Ipilimumab plus nivolumab is the most effective in prolonging PFS, but is far more toxic than nivolumab and pembrolizumab.
我们旨在比较并排序9种免疫检查点抑制剂相关疗法治疗晚期黑色素瘤的效果。
我们检索了PubMed、Cochrane数据库、科学网和ClinicalTrials.gov,以查找关于免疫检查点抑制剂相关治疗晚期黑色素瘤的随机对照试验。分析在贝叶斯框架下进行。
共识别出12项试验,涉及5413名患者。与伊匹单抗相比,伊匹单抗联合纳武单抗、纳武单抗和帕博利珠单抗在无进展生存期(PFS)方面显著更有效(风险比[HR]分别为0.38、0.50和0.58),与伊匹单抗联合化疗相比(分别为0.45、0.60和0.70),或与伊匹单抗联合沙格司亭相比(分别为0.44、0.57和0.67)。伊匹单抗联合gp100在PFS方面显著不如其余8种免疫检查点抑制剂相关策略有效。在改善总生存期(OS)方面,帕博利珠单抗显著比伊匹单抗和伊匹单抗联合gp100更有效(HR分别为0.66和0.64)。纳武单抗在OS方面显著优于曲美木单抗(HR为0.48)。就OS而言,伊匹单抗联合沙格司亭被列为第二有效的策略,且耐受性良好。纳武单抗和帕博利珠单抗显示出最佳的可接受性,与伊匹单抗相比(优势比[OR]分别为0.49和0.50)、曲美木单抗相比(分别为0.21和0.21)、伊匹单抗联合化疗相比(分别为0.13和0.13)或伊匹单抗联合纳武单抗相比(分别为0.15和0.15),高级别不良事件显著更少。
纳武单抗、帕博利珠单抗和伊匹单抗联合沙格司亭可能是晚期黑色素瘤的最佳治疗方法,因为它们在获益和可接受性之间具有最有利的平衡。伊匹单抗联合纳武单抗在延长PFS方面最有效,但毒性远高于纳武单抗和帕博利珠单抗。