Nandi Sulakshana, Schneider Helen, Dixit Priyanka
Public Health Resource Network, India, Raipur, Chhattisgarh, India.
School of Public Health, University of the Western Cape, Bellville, South Africa.
PLoS One. 2017 Nov 17;12(11):e0187904. doi: 10.1371/journal.pone.0187904. eCollection 2017.
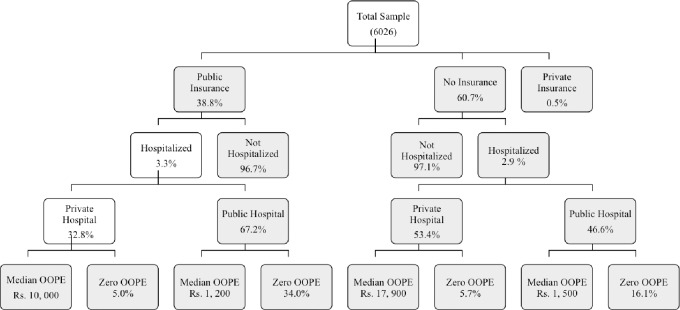
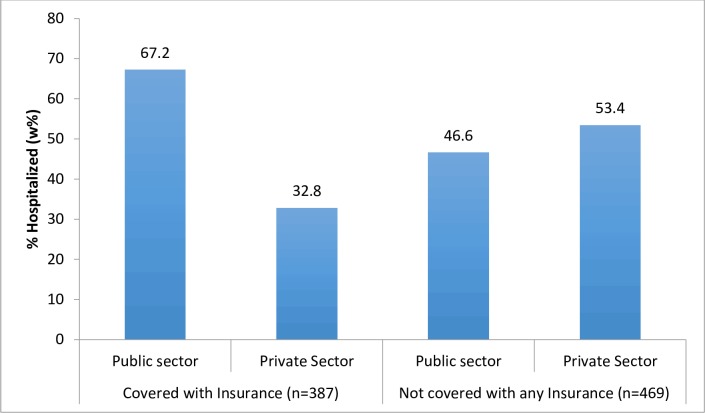
Research on impact of publicly financed health insurance has paid relatively little attention to the nature of healthcare provision the schemes engage. India's National Health Insurance Scheme or RSBY was made universal by Chhattisgarh State in 2012. In the State, public and private sectors provide hospital services in a context of extensive gender, social, economic and geographical inequities. This study examined enrolment, utilization (public and private) and out of pocket (OOP) expenditure for the insured and uninsured, in Chhattisgarh. The Chhattisgarh State Central sample (n = 6026 members) of the 2014 National Sample Survey (71st Round) on Health was extracted and analyzed. Variables of enrolment, hospitalization, out of pocket (OOP) expenditure and catastrophic expenditure were descriptively analyzed. Multivariate analyses of factors associated with enrolment, hospitalization (by sector) and OOP expenditure were conducted, taking into account gender, socio-economic status, residence, type of facility and ailment. Insurance coverage was 38.8%. Rates of hospitalization were 33/1000 population among the insured and 29/1000 among the uninsured. Of those insured and hospitalized, 67.2% utilized the public sector. Women, rural residents, Scheduled Tribes and poorer groups were more likely to utilize the public sector for hospitalizations. Although the insured were less likely to incur out of pocket (OOP) expenditure, 95.1% of insured private sector users and 66.0% of insured public sector users, still incurred costs. Median OOP payments in the private sector were eight times those in the public sector. Of households with at least one member hospitalized, 35.5% experienced catastrophic health expenditures (>10% monthly household consumption expenditure). The study finds that despite insurance coverage, the majority still incurred OOP expenditure. The public sector was nevertheless less expensive, and catered to the more vulnerable groups. It suggests the need to further examine the roles of public and private sectors in financial risk protection through government health insurance.
关于公共融资医疗保险影响的研究,相对较少关注这些计划所涉及的医疗服务提供的性质。印度的国家医疗保险计划或拉贾斯坦邦邦政府医疗保险计划(RSBY)于2012年由恰蒂斯加尔邦实现了普及。在该邦,公共部门和私营部门在广泛存在性别、社会、经济和地理不平等的背景下提供医院服务。本研究调查了恰蒂斯加尔邦参保者和未参保者的参保情况、医疗服务利用情况(公共部门和私营部门)以及自付费用。提取并分析了2014年全国卫生样本调查(第71轮)恰蒂斯加尔邦中央样本(n = 6026名成员)。对参保情况、住院治疗情况、自付费用和灾难性支出等变量进行了描述性分析。在考虑性别、社会经济地位、居住地、医疗机构类型和疾病的情况下,对与参保、住院治疗(按部门)和自付费用相关的因素进行了多变量分析。保险覆盖率为38.8%。参保者的住院率为每1000人中有33人,未参保者为每1000人中有29人。在参保并住院的人群中,67.2%利用了公共部门的服务。女性、农村居民、部落居民和较贫困群体更有可能在住院时利用公共部门的服务。尽管参保者自付费用的可能性较小,但95.1%的参保私营部门使用者和66.0%的参保公共部门使用者仍需承担费用。私营部门的自付费用中位数是公共部门的八倍。在至少有一名成员住院的家庭中,35.5%经历了灾难性医疗支出(超过家庭月消费支出的10%)。研究发现,尽管有保险覆盖,但大多数人仍需承担自付费用。不过,公共部门的费用较低,并为更弱势群体提供服务。这表明有必要进一步研究公共部门和私营部门在通过政府医疗保险提供财务风险保护方面的作用。