Division of Oral Health, Centers for Disease Control and Prevention (CDC), 4770 Buford HWY NE, MS-F80, Atlanta, GA 30341, United States.
Economic Research Service, US Department of Agriculture, 355 E Street, SW, Washington, DC 20024, United States.
Prev Med. 2018 Jun;111:291-298. doi: 10.1016/j.ypmed.2017.11.015. Epub 2017 Nov 16.
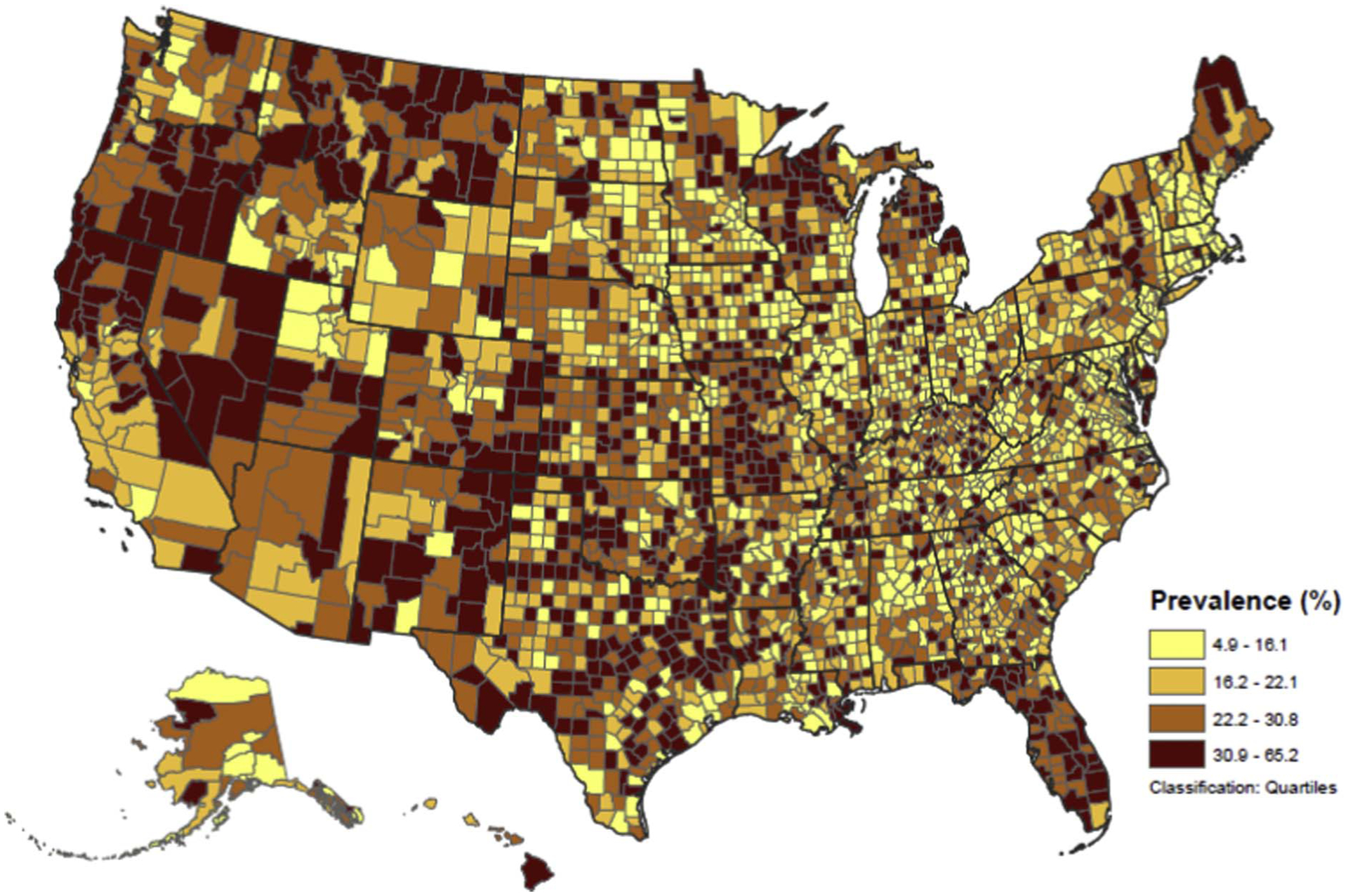
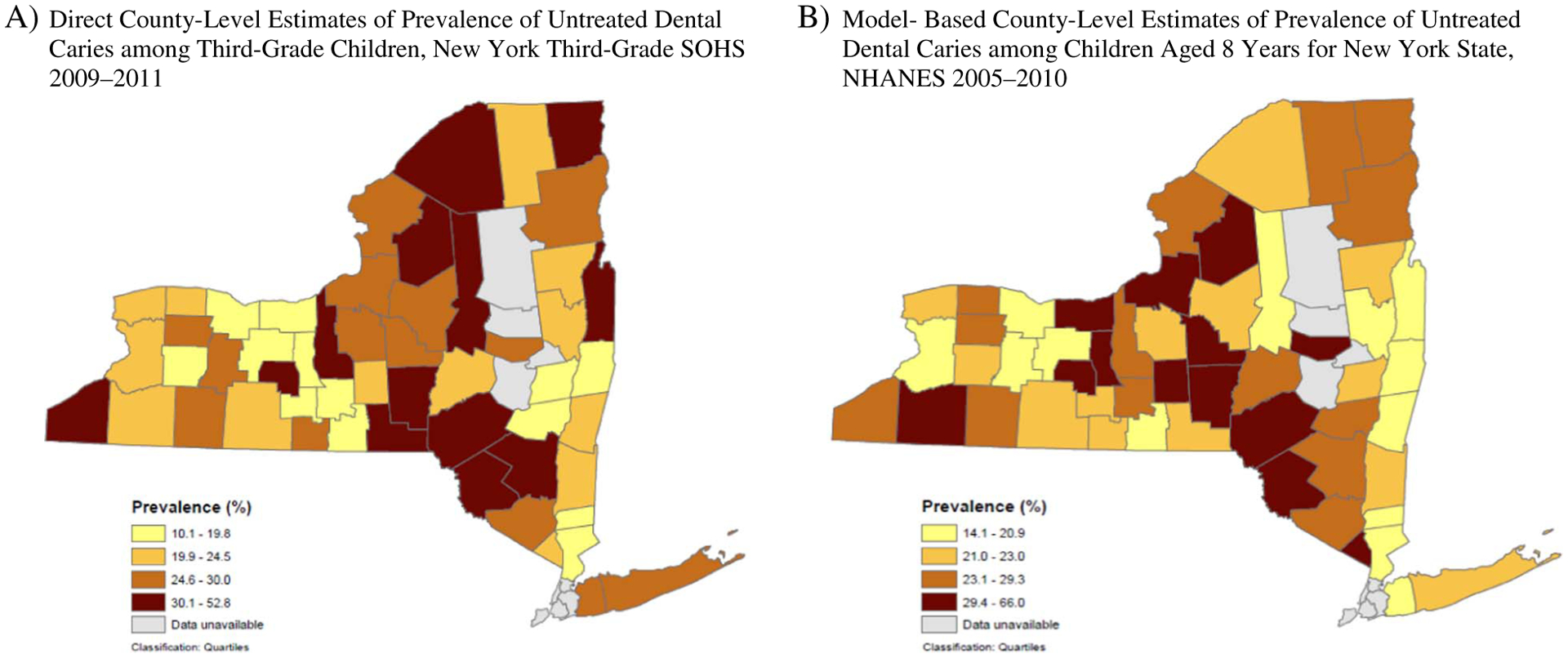
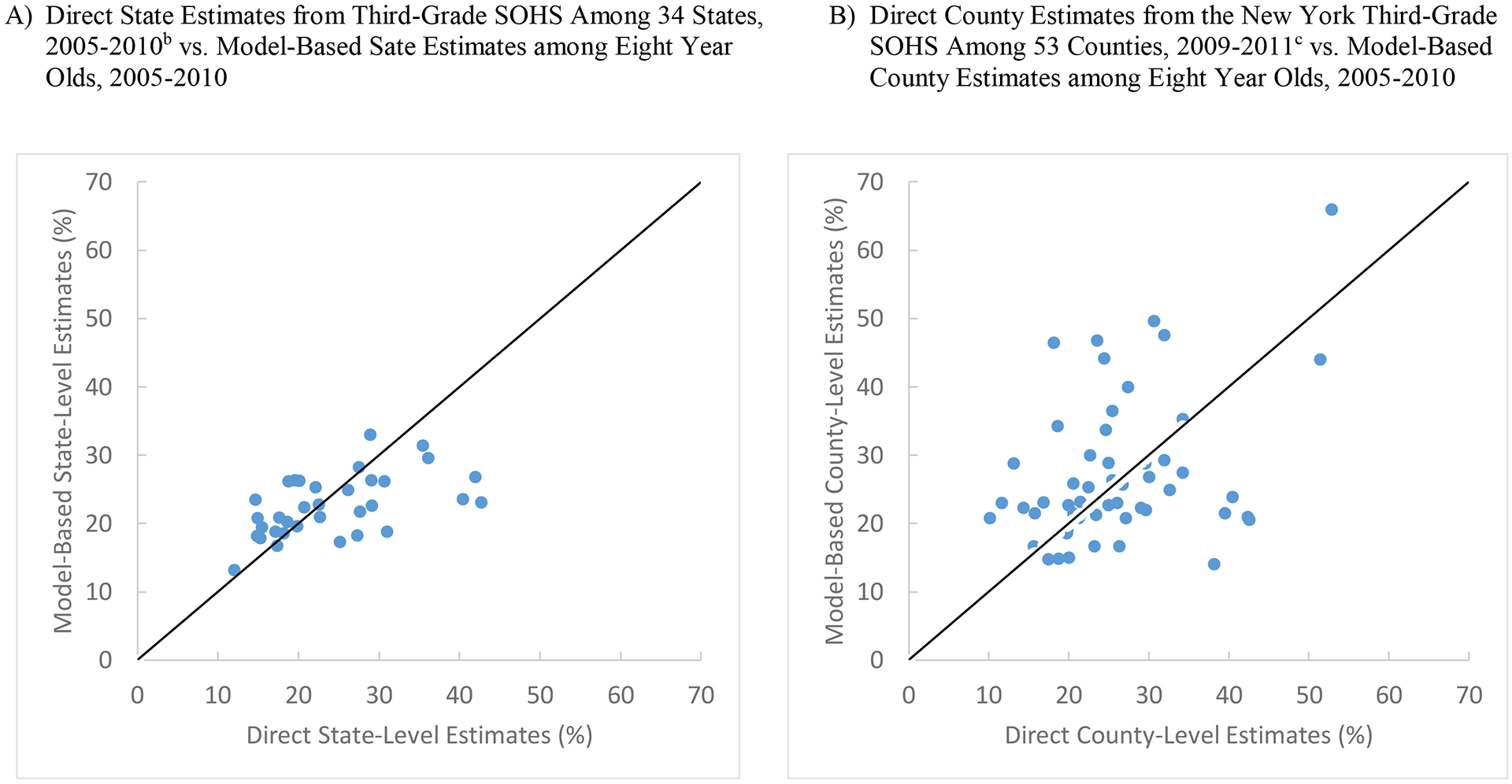
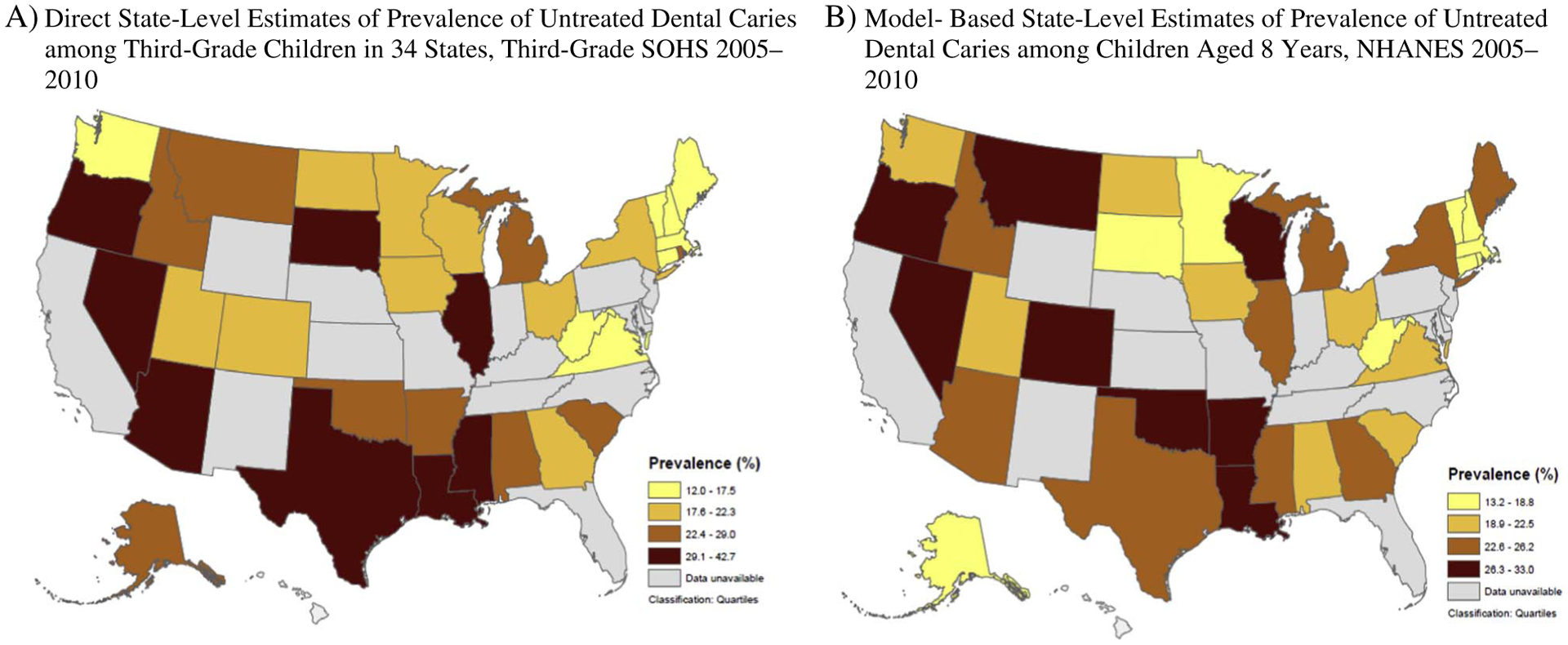
Because conducting population-based oral health screening is resource intensive, oral health data at small-area levels (e.g., county-level) are not commonly available. We applied the multilevel logistic regression and poststratification method to estimate county-level prevalence of untreated dental caries among children aged 6-9years in the United States using data from the National Health and Nutrition Examination Survey (NHANES) 2005-2010 linked with various area-level data at census tract, county and state levels. We validated model-based national estimates against direct estimates from NHANES. We also compared model-based estimates with direct estimates from select State Oral Health Surveys (SOHS) at state and county levels. The model with individual-level covariates only and the model with individual-, census tract- and county-level covariates explained 7.2% and 96.3% respectively of overall county-level variation in untreated caries. Model-based county-level prevalence estimates ranged from 4.9% to 65.2% with median of 22.1%. The model-based national estimate (19.9%) matched the NHANES direct estimate (19.8%). We found significantly positive correlations between model-based estimates for 8-year-olds and direct estimates from the third-grade State Oral Health Surveys (SOHS) at state level for 34 states (Pearson coefficient: 0.54, P=0.001) and SOHS estimates at county level for 53 New York counties (Pearson coefficient: 0.38, P=0.006). This methodology could be a useful tool to characterize county-level disparities in untreated dental caries among children aged 6-9years and complement oral health surveillance to inform public health programs especially when local-level data are not available although the lack of external validation due to data unavailability should be acknowledged.
由于开展基于人群的口腔健康筛查需要耗费大量资源,因此通常无法获得小区域(如县级)的口腔健康数据。我们应用多水平逻辑回归和后分层方法,利用来自美国国家健康和营养调查(NHANES)2005-2010 年的数据,并结合普查区、县和州各级的各种区域水平数据,估计 6-9 岁儿童未治疗龋齿的县水平流行率。我们将基于模型的全国估计值与 NHANES 的直接估计值进行了验证。我们还将基于模型的估计值与来自选定州口腔健康调查(SOHS)的州和县一级的直接估计值进行了比较。仅包含个体水平协变量的模型和包含个体、普查区和县级协变量的模型分别解释了未治疗龋齿的县一级总变异的 7.2%和 96.3%。基于模型的县一级流行率估计值范围为 4.9%至 65.2%,中位数为 22.1%。基于模型的全国估计值(19.9%)与 NHANES 的直接估计值(19.8%)相匹配。我们发现,对于 8 岁儿童,基于模型的估计值与来自 34 个州的三年级州口腔健康调查(SOHS)的直接估计值(Pearson 系数:0.54,P=0.001)和 53 个纽约县的 SOHS 县一级估计值(Pearson 系数:0.38,P=0.006)之间存在显著正相关关系。这种方法可以成为一种有用的工具,用于描述 6-9 岁儿童未治疗龋齿的县一级差异,并补充口腔健康监测,为公共卫生计划提供信息,特别是在无法获得地方一级数据的情况下,尽管由于数据不可用而缺乏外部验证应该得到承认。