Neuroscience and Aphasia Research Unit, University of Manchester, UK.
Neuroscience and Aphasia Research Unit, University of Manchester, UK.
Neuroimage Clin. 2017 Nov 6;17:465-473. doi: 10.1016/j.nicl.2017.10.037. eCollection 2018.
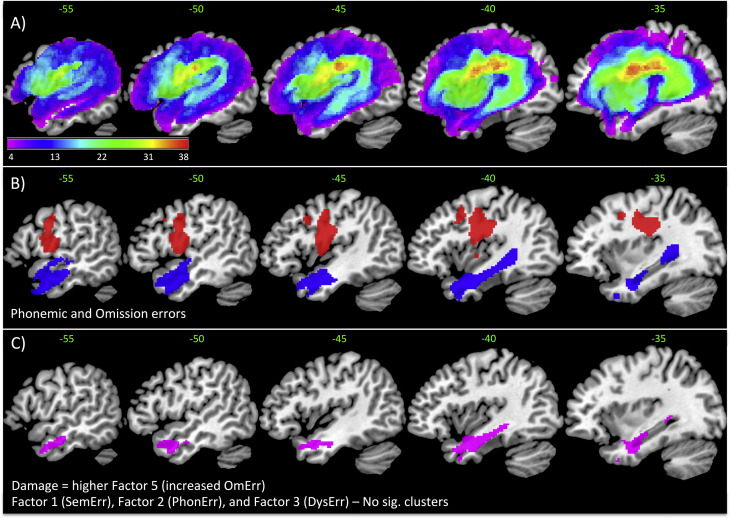
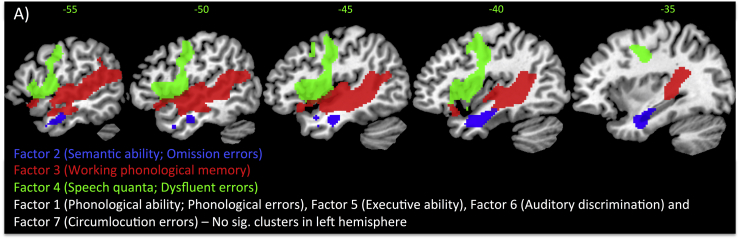
In order to gain a better understanding of aphasia one must consider the complex combinations of language impairments along with the pattern of paraphasias. Despite the fact that both deficits and paraphasias feature in diagnostic criteria, most research has focused only on the lesion correlates of language deficits, with minimal attention on the pattern of patients' paraphasias. In this study, we used a data-driven approach (principal component analysis - PCA) to fuse patient impairments and their pattern of errors into one unified model of chronic post-stroke aphasia. This model was subsequently mapped onto the patients' lesion profiles to generate the triangulation of language-cognitive impairments, naming errors and their neural correlates. Specifically, we established the pattern of co-occurrence between fifteen error types, which avoids focussing on a subset of errors or the use of experimenter-derived methods to combine across error types. We obtained five principal components underlying the patients' errors: omission errors; semantically-related responses; phonologically-related responses; dysfluent responses; and a combination of circumlocutions with mixed errors. In the second step, we aligned these paraphasia-related principal components with the patients' performance on a detailed language and cognitive assessment battery, utilising an additional PCA. This omnibus PCA revealed seven unique fused impairment-paraphasia factors: output phonology; semantics; phonological working memory; speech quanta; executive-cognitive skill; phonological (input) discrimination; and the production of circumlocution errors. In doing so we were able to resolve the complex relationships between error types and impairments. Some are relatively straightforward: circumlocution errors formed their own independent factor; there was a one-to-one mapping for phonological errors with expressive phonological abilities and for dysfluent errors with speech fluency. In contrast, omission-type errors loaded across both semantic and phonological working memory factors, whilst semantically-related errors had the most complex relationship by loading across four factors (phonological ability, speech quanta, executive-cognitive skills and circumlocution-type errors). Three components had unique lesion correlates: phonological working memory with the primary auditory region; semantics with the anterior temporal region; and fluency with the pre-central gyrus, converging with existing literature. In conclusion, the data-driven approach allowed derivation of the triangulation of deficits, error types and lesion correlates in post-stroke aphasia.
为了更好地理解失语症,必须考虑语言障碍的复杂组合以及错语的模式。尽管缺陷和错语都包含在诊断标准中,但大多数研究仅关注语言缺陷的病变相关性,而对患者错语的模式关注甚少。在这项研究中,我们使用了一种数据驱动的方法(主成分分析 - PCA)将患者的损伤及其错误模式融合到一个慢性中风后失语症的统一模型中。然后,将该模型映射到患者的病变谱上,生成语言-认知损伤、命名错误及其神经相关性的三角关系。具体来说,我们建立了 15 种错误类型之间的共现模式,避免了仅关注部分错误或使用实验者衍生的方法来跨错误类型进行组合。我们得到了患者错误的五个主要成分:遗漏错误;语义相关反应;语音相关反应;不流畅反应;以及迂回与混合错误的组合。在第二步中,我们利用附加的 PCA 将这些与错语相关的主要成分与患者在详细语言和认知评估测试中的表现对齐。这个综合 PCA 揭示了七个独特的融合损伤-错语因素:输出语音;语义;语音工作记忆;言语量子;执行认知技能;语音(输入)辨别;以及迂回错误的产生。通过这样做,我们能够解决错误类型和损伤之间的复杂关系。有些关系相对简单:迂回错误形成了自己独立的因素;语音错误与表达性语音能力之间存在一对一映射,不流畅错误与言语流畅性之间也存在映射。相比之下,遗漏型错误跨越语义和语音工作记忆两个因素加载,而语义相关错误通过加载四个因素(语音能力、言语量子、执行认知技能和迂回型错误)具有最复杂的关系。三个成分具有独特的病变相关性:语音工作记忆与初级听觉区域相关;语义与前颞叶区域相关;流畅性与中央前回相关,与现有文献一致。总之,数据驱动的方法允许在中风后失语症中得出损伤、错误类型和病变相关性的三角关系。