Department of Critical Care Medicine, Hoag Hospital, Newport Beach, CA, USA.
Department of Social and Decision Sciences, Carnegie Mellon University, Pittsburgh, PA, USA.
Med Decis Making. 2018 Apr;38(3):344-354. doi: 10.1177/0272989X17738958. Epub 2017 Nov 22.
Variation in the intensity of acute care treatment at the end of life is influenced more strongly by hospital and provider characteristics than patient preferences.
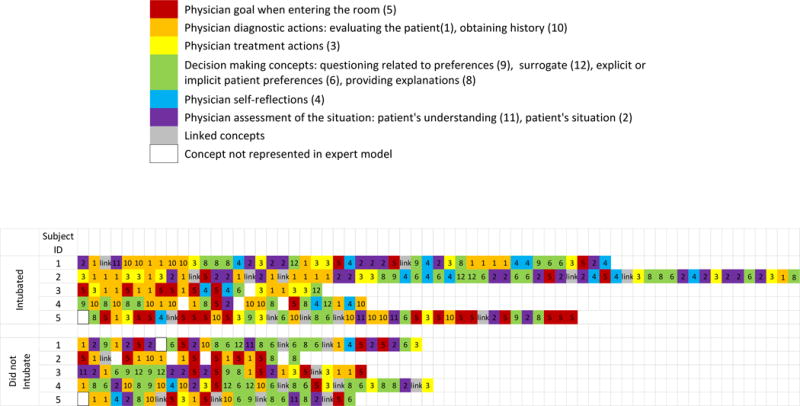
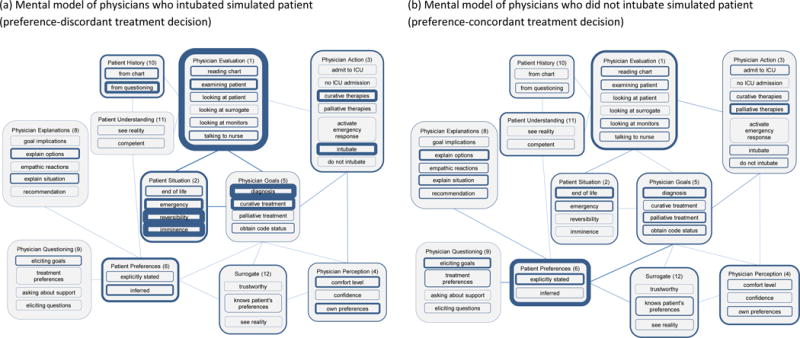
We sought to describe physicians' mental models (i.e., thought processes) when encountering a simulated critically and terminally ill older patient, and to compare those models based on whether their treatment plan was patient preference-concordant or preference-discordant.
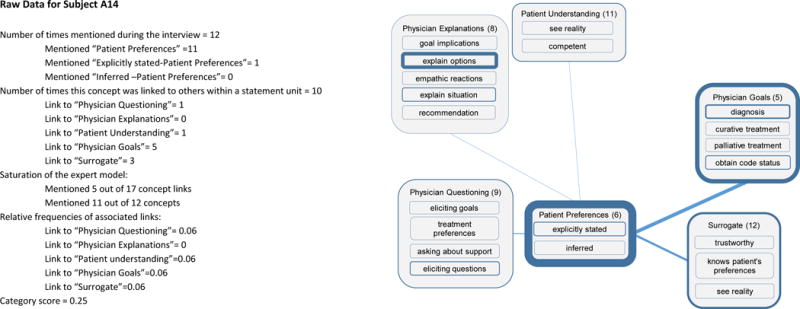
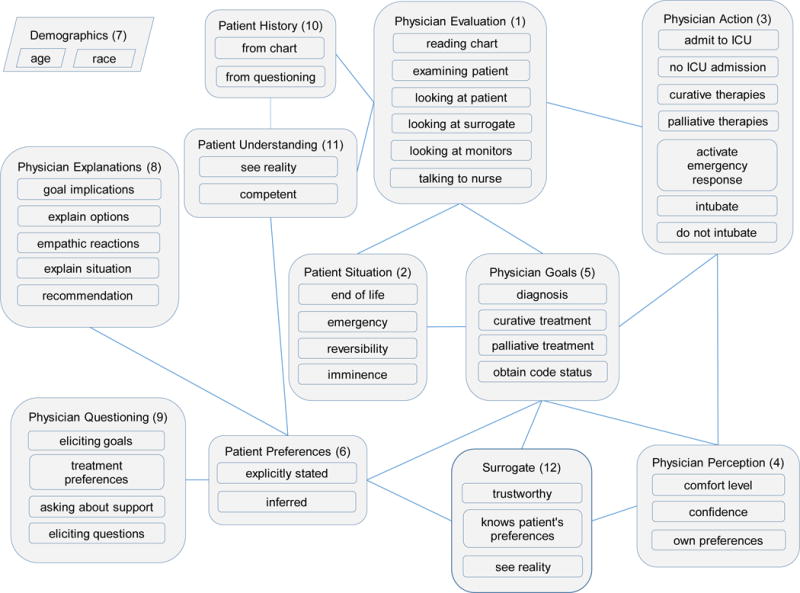
Seventy-three hospital-based physicians from 3 academic medical centers engaged in a simulated patient encounter and completed a mental model interview while watching the video recording of their encounter. We used an "expert" model to code the interviews. We then used Kruskal-Wallis tests to compare the weighted mental model themes of physicians who provided preference-concordant treatment with those who provided preference-discordant treatment.
Sixty-six (90%) physicians provided preference-concordant treatment and 7 (10%) provided preference-discordant treatment (i.e., they intubated the patient). Physicians who intubated the patient were more likely to emphasize the reversible and emergent nature of the patient situation (z = -2.111, P = 0.035), their own comfort (z = -2.764, P = 0.006), and rarely focused on explicit patient preferences (z = 2.380, P = 0.017).
Post-decisional interviewing with audio/video prompting may induce hindsight bias. The expert model has not yet been validated and may not be exhaustive. The small sample size limits generalizability and power.
Hospital-based physicians providing preference-discordant used a different mental model for decision making for a critically and terminally ill simulated case. These differences may offer targets for future interventions to promote preference-concordant care for seriously ill patients.
在生命末期,急性治疗强度的变化受医院和提供者特征的影响比患者偏好更为强烈。
我们旨在描述医生在遇到模拟的重症和终末期老年患者时的思维模式(即思维过程),并根据他们的治疗计划是否与患者偏好一致或不一致来比较这些模式。
来自 3 家学术医疗中心的 73 名医院医生参与了模拟患者就诊,并在观看就诊录像的同时完成了思维模式访谈。我们使用“专家”模型对访谈进行编码。然后,我们使用 Kruskal-Wallis 检验比较提供偏好一致治疗的医生和提供偏好不一致治疗的医生的加权思维模式主题。
66 名(90%)医生提供了偏好一致的治疗,7 名(10%)医生提供了偏好不一致的治疗(即他们对患者进行了插管)。对患者进行插管的医生更倾向于强调患者情况的可逆性和紧急性(z=-2.111,P=0.035)、自身的舒适度(z=-2.764,P=0.006),很少关注明确的患者偏好(z=2.380,P=0.017)。
事后访谈与音频/视频提示可能会引起后见之明偏差。专家模型尚未经过验证,可能并不详尽。样本量小限制了普遍性和功效。
提供偏好不一致治疗的医院医生在决策重症和终末期模拟病例时使用了不同的思维模式。这些差异可能为未来促进重病患者偏好一致护理的干预措施提供目标。