Hormone Laboratory, Haukeland University Hospital, Bergen, Norway.
Department of Clinical Science, University of Bergen, Bergen, Norway.
Breast Cancer Res. 2017 Nov 28;19(1):125. doi: 10.1186/s13058-017-0916-4.
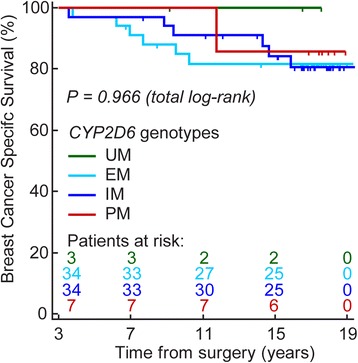
Controversies exist as to whether the genetic polymorphisms of the enzymes responsible for the metabolism of tamoxifen can predict breast cancer outcome in patients using adjuvant tamoxifen. Direct measurement of concentrations of active tamoxifen metabolites in serum may be a more biological plausible and robust approach. We have investigated the association between CYP2D6 genotypes, serum concentrations of active tamoxifen metabolites, and long-term outcome in tamoxifen treated breast cancer patients.
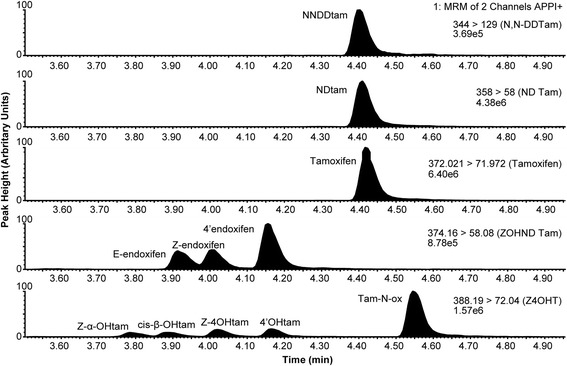
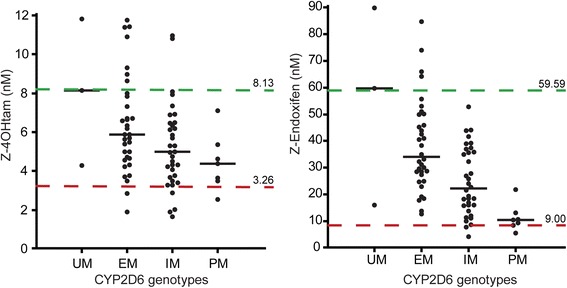
From an original observational study comprising 817 breast cancer patients, 99 women with operable breast cancer were retrospectively included in the present study. This cohort of patients were adjuvantly treated with tamoxifen, had provided serum samples suitable for measuring tamoxifen metabolites, and were relapse-free at 3 years after the primary treatment commenced. The median follow-up time from this entry point to breast cancer death was 13.9 years. Patients were CYP2D6 genotyped and grouped into four CYP2D6 phenotype groups (Ultra rapid, extensive, intermediate, and poor metabolizers). Tamoxifen and nine metabolites were quantified in serum (n = 86) and compared with CYP2D6 phenotype groups and outcome.
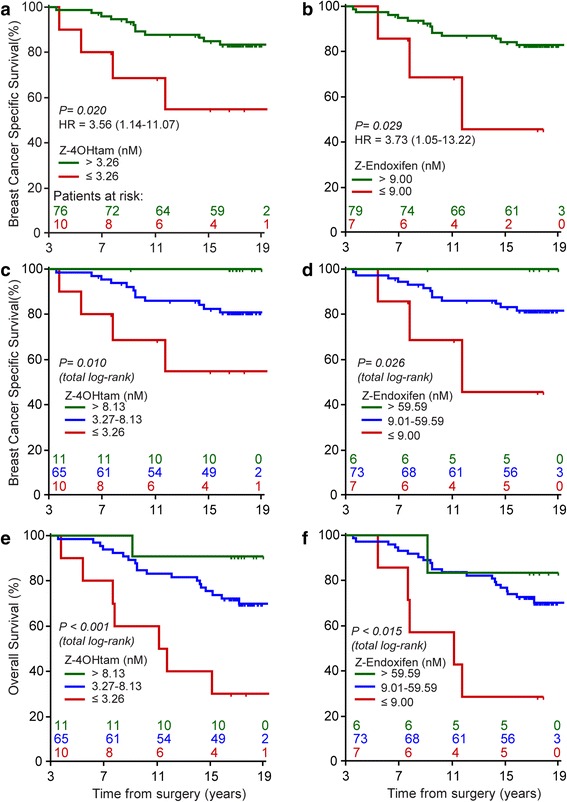
Breast cancer patients with low concentrations of Z-4-hydroxy-tamoxifen (Z-4OHtam; ≤ 3.26 nM) had a breast cancer-specific survival (BCSS) of 60% compared to 84% in patients with Z-4OHtam concentrations > 3.26 nM (p = 0.020, log-rank hazard ratio (HR) = 3.56, 95% confidence interval (CI) = 1.14-11.07). For patients with Z-4-hydroxy-N-desmethyl-tamoxifen (Z-endoxifen) levels ≤ 9.00 nM BCSS was 57% compared to 84% for patients with concentrations > 9.00 nM (p = 0.029, HR = 3.73, 95% CI = 1.05-13.22). Low concentrations of Z-4OHtam and Z-endoxifen were associated with poorer survival also after adjusting for clinically relevant variables (HR = 4.27, 95% CI = 1.35-13.58, and HR = 3.70, 95% CI = 1.03-13.25, respectively). Overall survival analysis showed similar survival differences for both active metabolites. The Antiestrogen Activity Score showed comparable effects, but did not improve the prognostic information.
Patients with Z-4OHtam and Z-endoxifen concentrations lower than 3.26 nM or 9.00 nM, respectively, showed an adverse outcome. Our results suggest that direct measurement of active tamoxifen metabolite concentrations could be of clinical value. Validation in larger study cohorts is warranted.
对于负责他莫昔芬代谢的酶的遗传多态性是否可以预测接受辅助他莫昔芬治疗的乳腺癌患者的乳腺癌结局,存在争议。直接测量血清中活性他莫昔芬代谢物的浓度可能是一种更具生物学合理性和稳健的方法。我们研究了 CYP2D6 基因型、血清中活性他莫昔芬代谢物浓度与接受他莫昔芬治疗的乳腺癌患者长期结局之间的关系。
从一项包含 817 例乳腺癌患者的原始观察性研究中,回顾性纳入了 99 例可手术乳腺癌患者参加本研究。这组患者接受他莫昔芬辅助治疗,提供了适合测量他莫昔芬代谢物的血清样本,并且在主要治疗开始后 3 年内无复发。从这个入组点到乳腺癌死亡的中位随访时间为 13.9 年。对患者进行 CYP2D6 基因分型,并分为四个 CYP2D6 表型组(超快、广泛、中间和弱代谢者)。对血清中的他莫昔芬和九种代谢物进行了定量(n=86),并与 CYP2D6 表型组和结局进行了比较。
Z-4-羟基他莫昔芬(Z-4OHtam)浓度低的乳腺癌患者(Z-4OHtam ≤ 3.26 nM)的乳腺癌特异性生存率(BCSS)为 60%,而 Z-4OHtam 浓度>3.26 nM 的患者为 84%(p=0.020,对数秩危险比(HR)=3.56,95%置信区间(CI)=1.14-11.07)。Z-4-羟基-N-去甲基他莫昔芬(Z-endoxifen)浓度≤9.00 nM 的患者的 BCSS 为 57%,而浓度>9.00 nM 的患者为 84%(p=0.029,HR=3.73,95%CI=1.05-13.22)。即使调整了临床相关变量,Z-4OHtam 和 Z-endoxifen 的低浓度也与较差的生存相关(HR=4.27,95%CI=1.35-13.58,HR=3.70,95%CI=1.03-13.25)。总生存分析显示两种活性代谢物均有类似的生存差异。抗雌激素活性评分显示出类似的效果,但没有改善预后信息。
Z-4OHtam 和 Z-endoxifen 浓度分别低于 3.26 nM 或 9.00 nM 的患者,其结局不良。我们的结果表明,直接测量活性他莫昔芬代谢物的浓度可能具有临床价值。需要在更大的研究队列中进行验证。