Division of Trauma and Critical Care, Department of Surgery, School of Medicine, University of Washington, Seattle, Washington.
Department of Surgery, Denver Health Medical Center, University of Colorado, Denver, Colorado.
Shock. 2018 Sep;50(3):258-264. doi: 10.1097/SHK.0000000000001073.
The Pragmatic Randomized Optimal Platelet and Plasma Ratios (PROPPR) study evaluated the effects of plasma and platelets on hemostasis and mortality after hemorrhage. The pulmonary consequences of resuscitation strategies that mimic whole blood, remain unknown.
A secondary analysis of the PROPPR study was performed. Injured patients predicted to receive a massive transfusion were randomized to 1:1:1 versus 1:1:2 plasma-platelet-red blood cell ratios at 12 Level I North American trauma centers. Patients with survival >24 h, an intensive care unit (ICU) stay, and a recorded PaO2/FiO2 (P/F) ratio were included. Acute respiratory distress syndrome (ARDS) was defined as a P/F ratio < 200, with bilateral pulmonary infiltrates, and adjudicated by investigators.
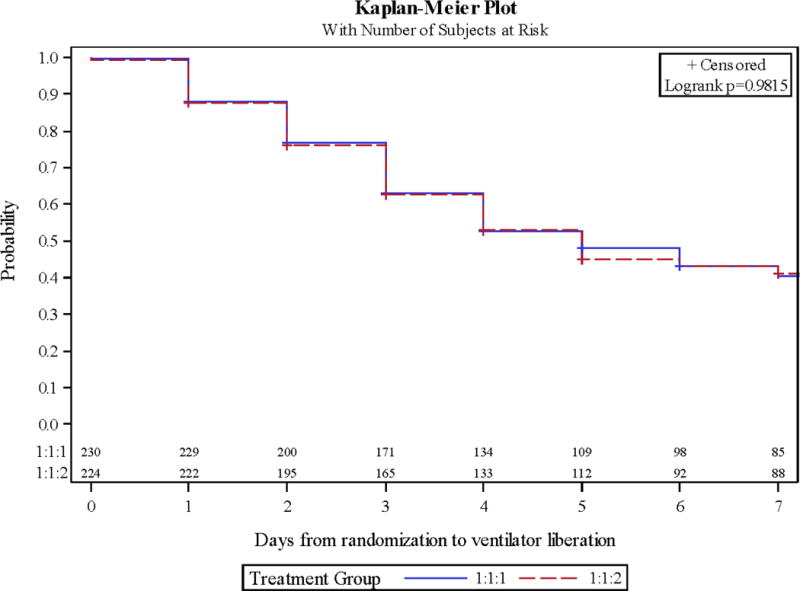
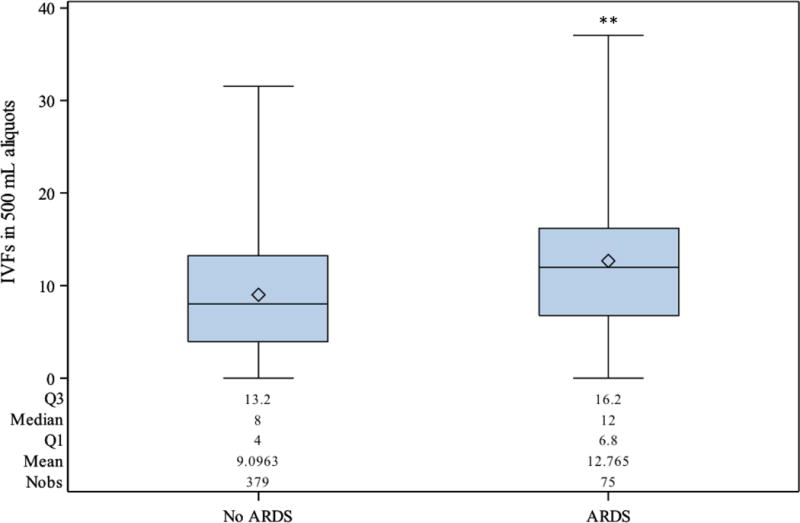
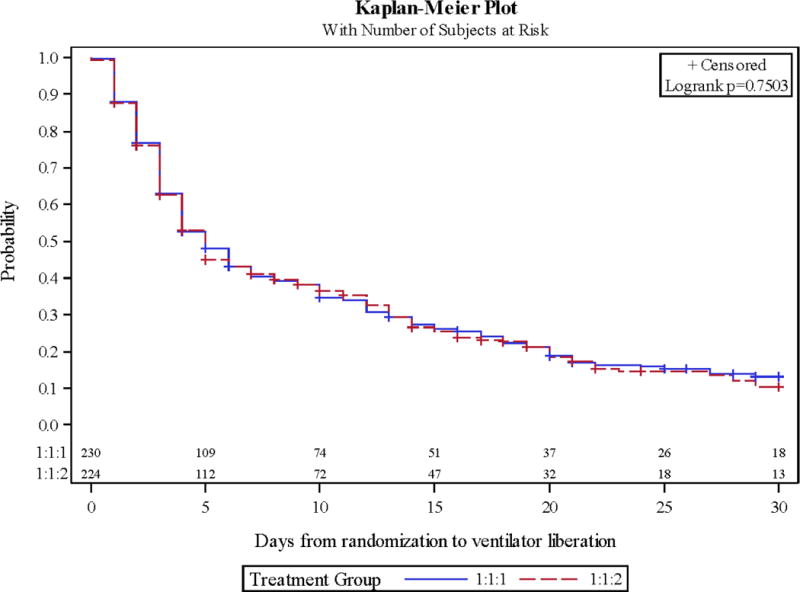
Four hundred fifty-four patients were reviewed (230 received 1:1:1, 224 1:1:2). Age, sex, injury mechanism, and regional abbreviated injury scale (AIS) scores did not differ between cohorts. Tidal volume, positive end-expiratory pressure, and lowest P/F ratio did not differ. No significant differences in ARDS rates (14.8% vs. 18.4%), ventilator-free (24 vs. 24) or ICU-free days (17.5 vs. 18), hospital length of stay (22 days vs. 18 days), or 30-day mortality were found (28% vs. 28%). ARDS was associated with blunt injury (OR 3.61 [1.53-8.81] P < 0.01) and increasing chest AIS (OR 1.40 [1.15-1.71] P < 0.01). Each 500 mL of crystalloid infused during hours 0 to 6 was associated with a 9% increase in the rate of ARDS (OR 1.09 [1.04-1.14] P < 0.01). Blood given at 0 to 6 or 7 to 24 h were not risk factors for lung injury.
Acute crystalloid exposure, but not blood products, is a potentially modifiable risk factor for the prevention of ARDS following hemorrhage.
随机、实用、优化血小板与血浆比例研究(PROPPR 研究)评估了出血后血液凝固和死亡率的血浆和血小板作用。目前仍不清楚模拟全血复苏策略对肺的影响。
对 PROPPR 研究进行二次分析。在 12 个北美一级创伤中心,预计接受大量输血的受伤患者被随机分为 1:1:1 与 1:1:2 的血浆-血小板-红细胞比例。纳入生存时间>24 小时、入住重症监护病房(ICU)且记录有动脉血氧分压/吸氧浓度(PaO2/FiO2)比值的患者。急性呼吸窘迫综合征(ARDS)的定义为 PaO2/FiO2 比值<200、有双侧肺部浸润,并由研究者进行评估。
共回顾了 454 例患者(1:1:1 组 230 例,1:1:2 组 224 例)。两组患者的年龄、性别、损伤机制和区域简明损伤评分(AIS)无差异。潮气量、呼气末正压和最低 PaO2/FiO2 比值无差异。ARDS 发生率(14.8%比 18.4%)、无呼吸机天数(24 比 24)、无 ICU 天数(17.5 比 18)、住院时间(22 天比 18 天)或 30 天死亡率(28%比 28%)无显著差异。钝伤(比值比 3.61[1.53-8.81],P<0.01)和胸部 AIS 增加(比值比 1.40[1.15-1.71],P<0.01)与 ARDS 相关。伤后 0 至 6 小时输注的每 500ml 晶体液与 ARDS 发生率增加 9%相关(比值比 1.09[1.04-1.14],P<0.01)。伤后 0 至 6 小时或 7 至 24 小时给予的血液制品不是肺部损伤的危险因素。
急性晶体液暴露,而非血液制品,是出血后预防 ARDS 的一个潜在可改变的危险因素。