Department of Cardiology and Cardiovascular Medicine, University Hospital Eberhard Karls University Tuebingen, Tuebingen, Germany.
Department of Anesthesiology, University Hospital Eberhard Karls University Tuebingen, Tuebingen, Germany.
J Am Heart Assoc. 2017 Dec 2;6(12):e007485. doi: 10.1161/JAHA.117.007485.
Percutaneous edge-to-edge mitral valve repair (PMVR) has become an established treatment option for mitral regurgitation in patients not eligible for surgical repair. Currently, most procedures are performed under general anesthesia (GA). An increasing number of centers, however, are performing the procedure under deep sedation (DS). Here, we compared patients undergoing PMVR with GA or DS.
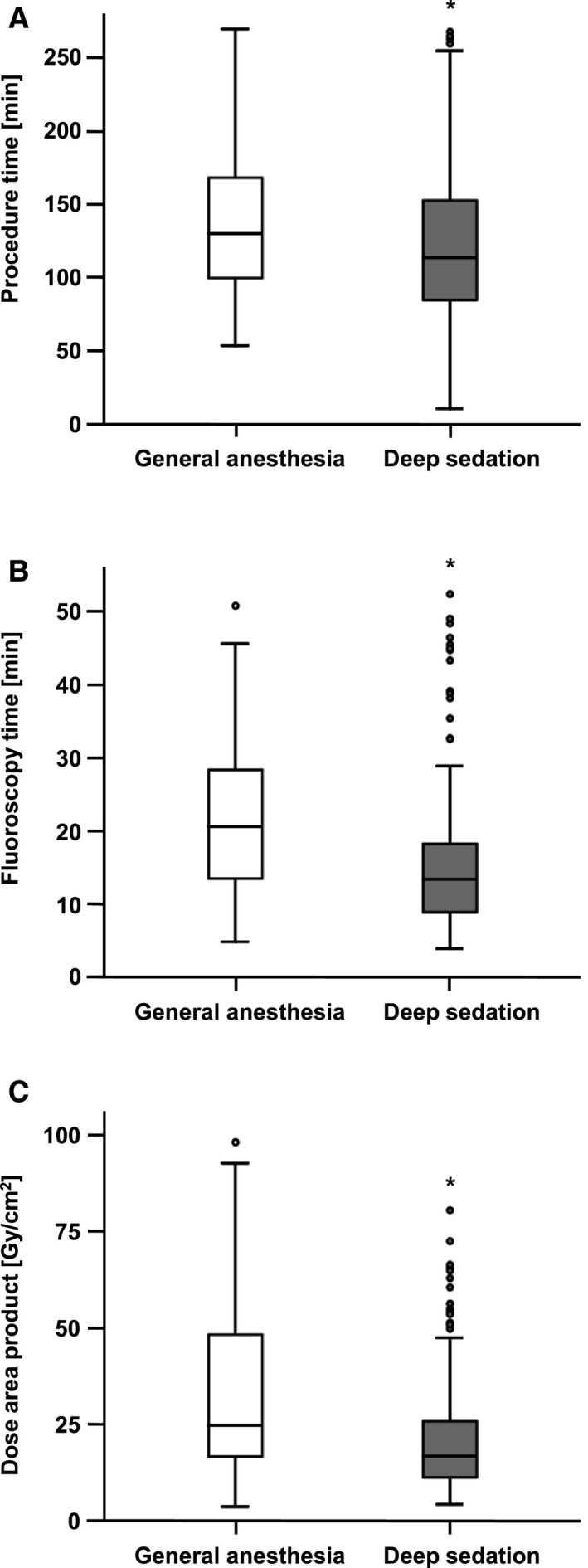
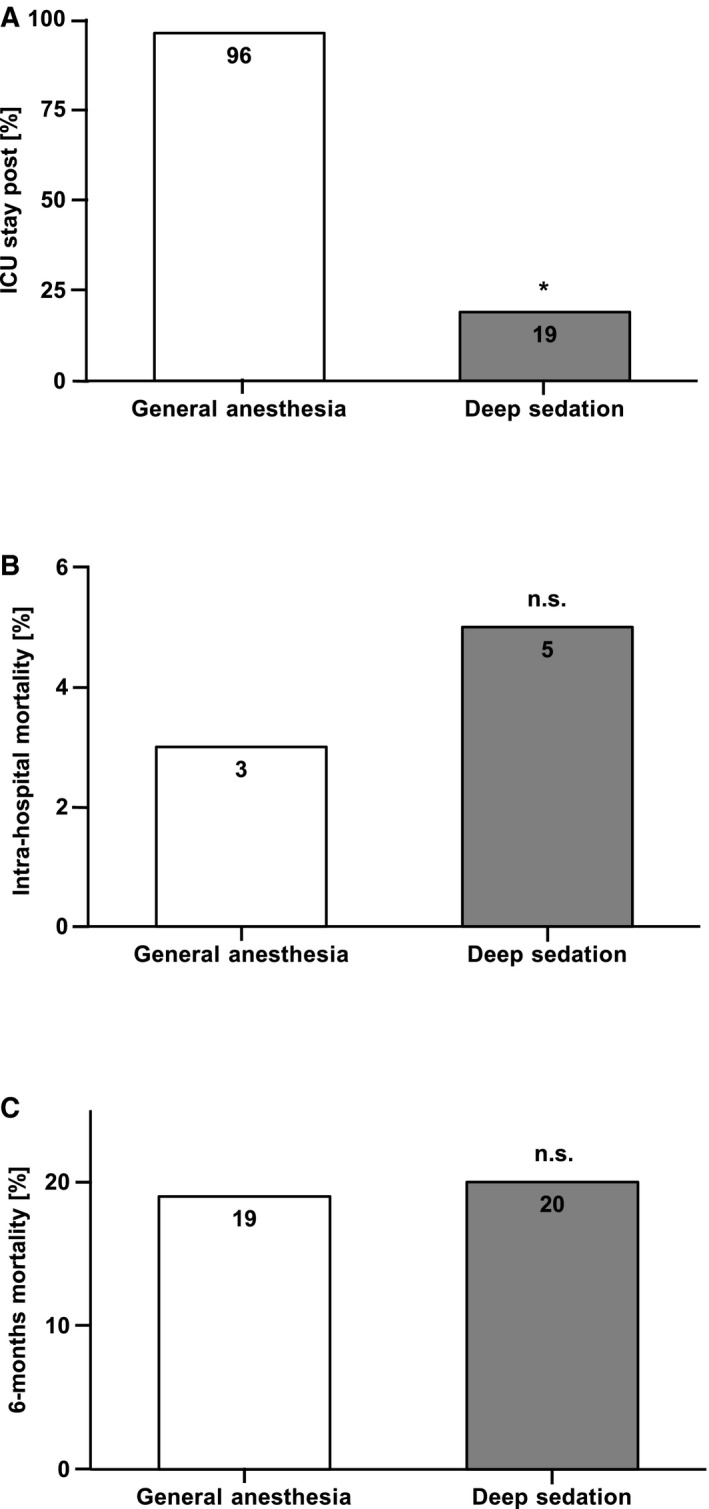
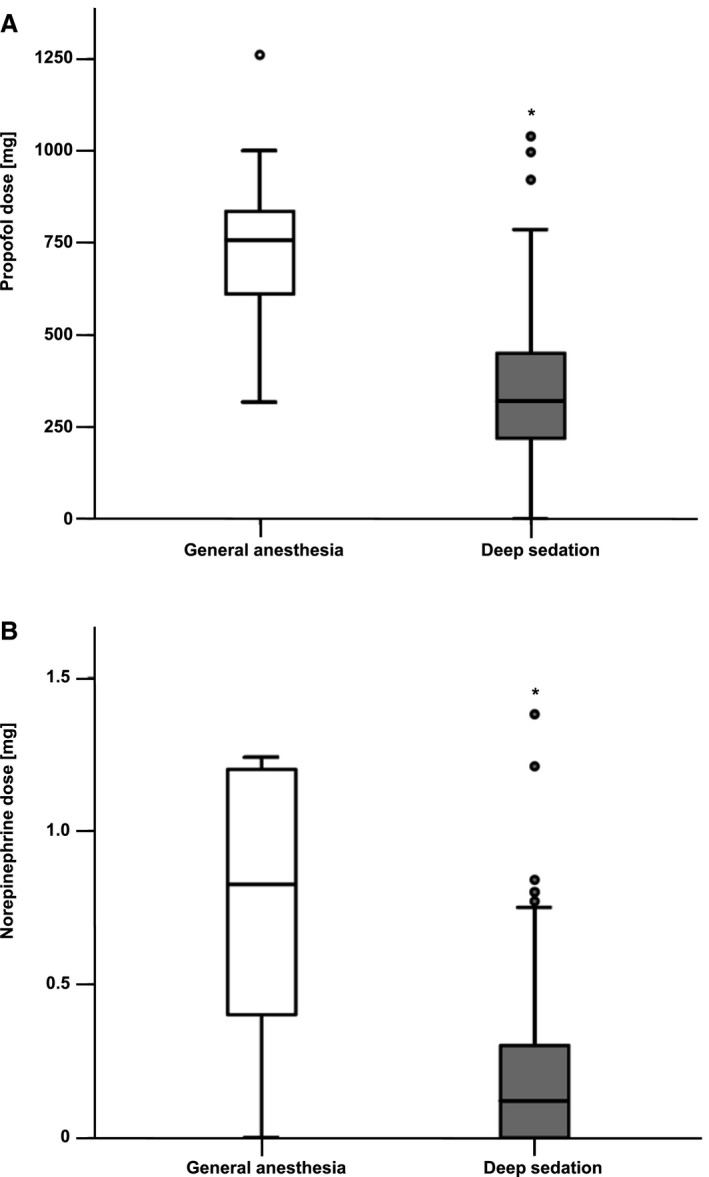
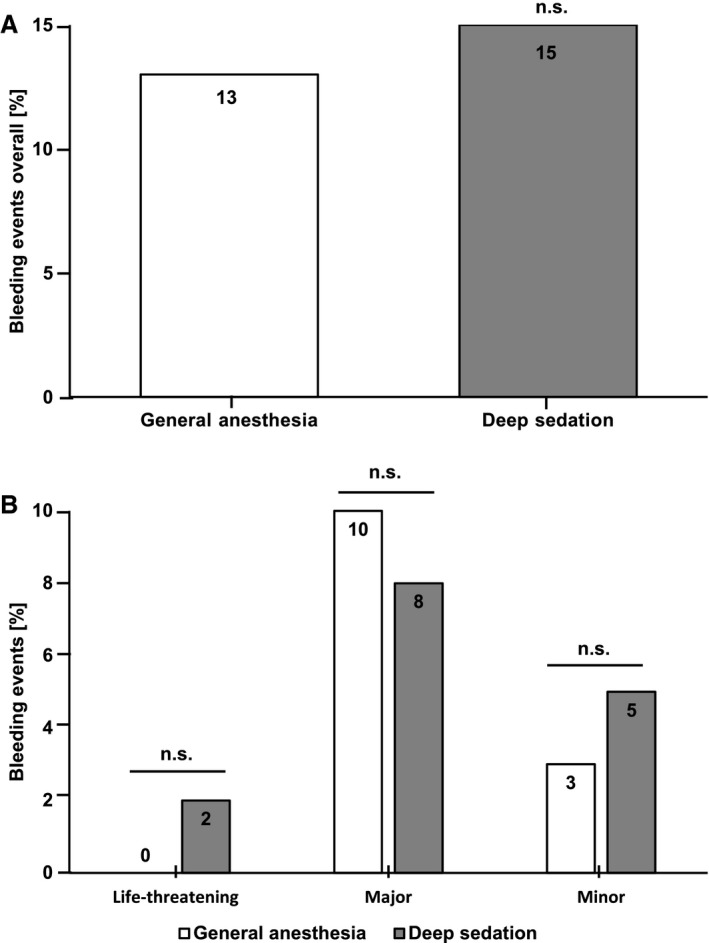
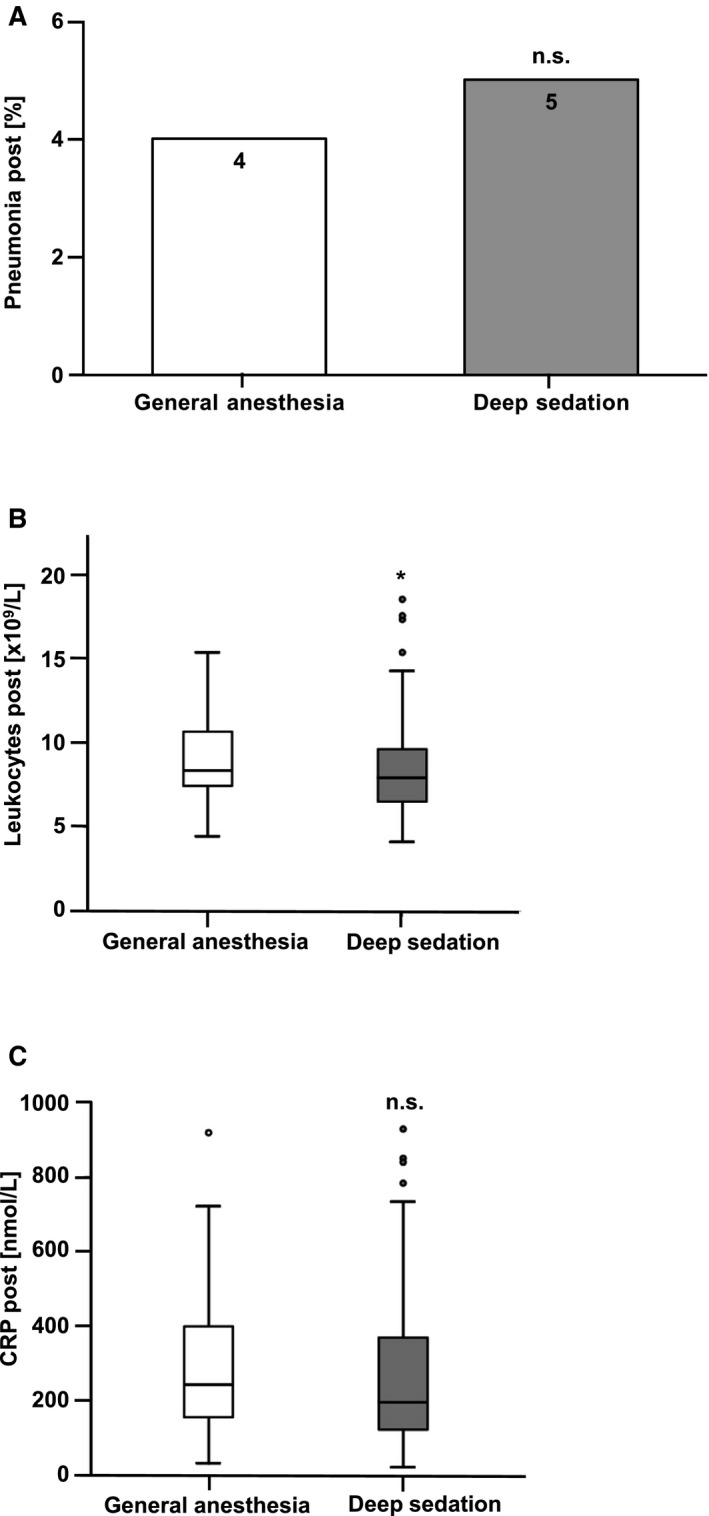
A total of 271 consecutive patients underwent PMVR at our institution between May 2014 and December 2016. Seventy-two procedures were performed under GA and 199 procedures under DS. We observed that in the DS group, doses of propofol (743±228 mg for GA versus 369±230 mg for DS, <0.001) and norepinephrine (1.1±1.6 mg for GA versus 0.2±0.3 mg for DS, <0.001) were significantly lower. Procedure time, fluoroscopy time, and dose area product were significantly higher in the GA group. There was no significant difference between GA and DS with respect to overall bleeding complications, postinterventional pneumonia (4% for GA versus 5% for DS), or C-reactive protein levels (361±351 nmol/L for GA versus 278±239 nmol/L for DS). Significantly fewer patients with DS needed a postinterventional stay in the intensive care unit (96% for GA versus 19% for DS, <0.001). Importantly, there was no significant difference between DS and GA regarding intrahospital or 6-month mortality.
DS for PMVR is safe and feasible. No disadvantages with respect to procedural outcome or complications in comparison to GA were observed. Applying DS may simplify the PMVR procedure.
经皮缘对缘二尖瓣修复术(PMVR)已成为不能进行手术修复的二尖瓣反流患者的一种既定治疗选择。目前,大多数手术是在全身麻醉(GA)下进行的。然而,越来越多的中心正在在深度镇静(DS)下进行该手术。在这里,我们比较了在 GA 或 DS 下进行 PMVR 的患者。
在我们机构,2014 年 5 月至 2016 年 12 月期间,共有 271 例连续患者接受了 PMVR。72 例手术在 GA 下进行,199 例手术在 DS 下进行。我们观察到,在 DS 组中,丙泊酚的剂量(GA 组为 743±228mg,DS 组为 369±230mg,<0.001)和去甲肾上腺素的剂量(GA 组为 1.1±1.6mg,DS 组为 0.2±0.3mg,<0.001)明显较低。GA 组的手术时间、透视时间和剂量面积乘积明显较高。GA 和 DS 在总体出血并发症、介入后肺炎(GA 组为 4%,DS 组为 5%)或 C-反应蛋白水平(GA 组为 361±351nmol/L,DS 组为 278±239nmol/L)方面无显著差异。DS 组需要入住重症监护病房的患者明显较少(GA 组为 96%,DS 组为 19%,<0.001)。重要的是,DS 和 GA 在心内或 6 个月死亡率方面无显著差异。
PMVR 中的 DS 是安全且可行的。与 GA 相比,在手术结果或并发症方面没有观察到明显的不利之处。应用 DS 可能会简化 PMVR 程序。