IRCCS Don Gnocchi Foundation Onlus, Milan, Italy.
IRCCS Istituto di Ricerche Farmacologiche Mario Negri, Milan, Italy.
PLoS One. 2017 Dec 4;12(12):e0188642. doi: 10.1371/journal.pone.0188642. eCollection 2017.
Motor recovery of persons after stroke may be enhanced by a novel approach where residual muscle activity is facilitated by patient-controlled electrical muscle activation. Myoelectric activity from hemiparetic muscles is then used for continuous control of functional electrical stimulation (MeCFES) of same or synergic muscles to promote restoration of movements during task-oriented therapy (TOT). Use of MeCFES during TOT may help to obtain a larger functional and neurological recovery than otherwise possible.
Multicenter randomized controlled trial.
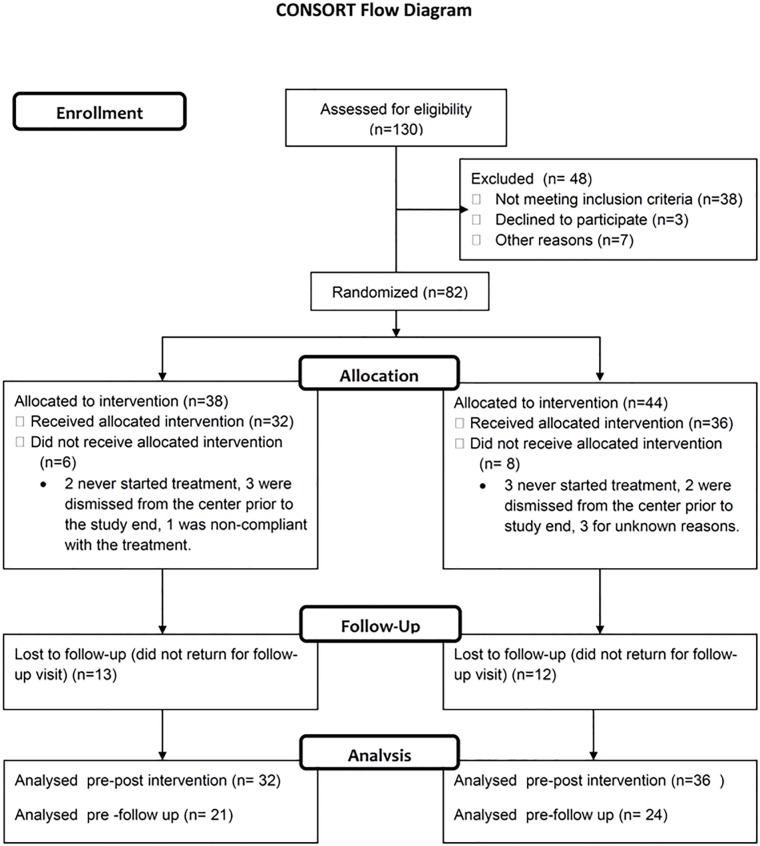
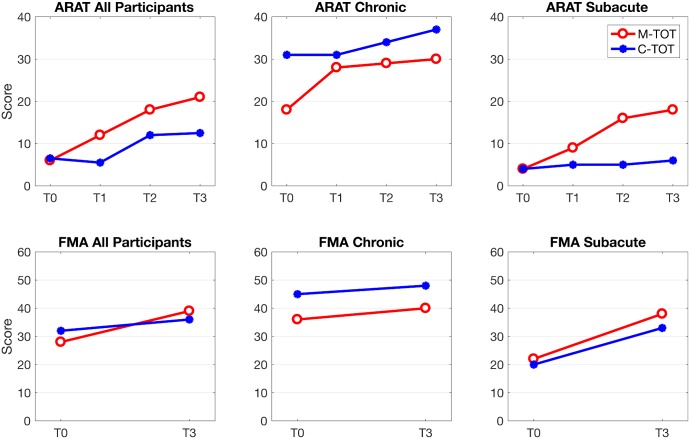
Eighty two acute and chronic stroke victims were recruited through the collaborating facilities and after signing an informed consent were randomized to receive either the experimental (MeCFES assisted TOT (M-TOT) or conventional rehabilitation care including TOT (C-TOT). Both groups received 45 minutes of rehabilitation over 25 sessions. Outcomes were Action Research Arm Test (ARAT), Upper Extremity Fugl-Meyer Assessment (FMA-UE) scores and Disability of the Arm Shoulder and Hand questionnaire.
Sixty eight subjects completed the protocol (Mean age 66.2, range 36.5-88.7, onset months 12.7, range 0.8-19.1) of which 45 were seen at follow up 5 weeks later. There were significant improvements in both groups on ARAT (median improvement: MeCFES TOT group 3.0; C-TOT group 2.0) and FMA-UE (median improvement: M-TOT 4.5; C-TOT 3.5). Considering subacute subjects (time since stroke < 6 months), there was a trend for a larger proportion of improved patients in the M-TOT group following rehabilitation (57.9%) than in the C-TOT group (33.2%) (difference in proportion improved 24.7%; 95% CI -4.0; 48.6), though the study did not meet the planned sample size.
This is the first large multicentre RCT to compare MeCFES assisted TOT with conventional care TOT for the upper extremity. No adverse events or negative outcomes were encountered, thus we conclude that MeCFES can be a safe adjunct to rehabilitation that could promote recovery of upper limb function in persons after stroke, particularly when applied in the subacute phase.
通过一种新方法,即通过患者控制的电肌肉激活来促进残留肌肉活动,从而增强中风后患者的运动恢复。然后,使用偏瘫肌肉的肌电活动对相同或协同肌肉进行连续控制的功能性电刺激(MeCFES),以促进任务导向治疗(TOT)期间运动的恢复。在 TOT 期间使用 MeCFES 可能有助于获得比其他情况下更大的功能和神经恢复。
多中心随机对照试验。
通过合作机构招募 82 名急性和慢性中风患者,并在签署知情同意书后随机分为实验组(MeCFES 辅助 TOT(M-TOT)或常规康复治疗,包括 TOT(C-TOT)。两组均接受 25 次 45 分钟的康复治疗。结果是使用动作研究上肢测试(ARAT)、上肢 Fugl-Meyer 评估(FMA-UE)评分和上肢残疾问卷。
68 名受试者完成了方案(平均年龄 66.2,范围 36.5-88.7,发病时间 12.7,范围 0.8-19.1),其中 45 名在 5 周后随访时出现。两组在 ARAT(中位改善:MeCFES TOT 组 3.0;C-TOT 组 2.0)和 FMA-UE(中位改善:M-TOT 4.5;C-TOT 3.5)方面均有显著改善。考虑到亚急性患者(中风后时间<6 个月),在康复后,M-TOT 组中改善患者的比例有较大趋势(57.9%)高于 C-TOT 组(33.2%)(改善比例差异 24.7%;95%CI-4.0;48.6%),尽管该研究未达到计划的样本量。
这是第一项比较 MeCFES 辅助 TOT 与常规 TOT 治疗上肢的大型多中心 RCT。未出现不良事件或负面结果,因此我们得出结论,MeCFES 可以作为康复的安全辅助手段,可促进中风后患者上肢功能的恢复,特别是在亚急性期应用时。