Kim Min Joon, Lee Ji Hwan, Jang Jo Ung, Quan Fu Shi, Kim Sun Kwang, Kim Woojin
Department of East-West Medicine, Graduate School, Kyung Hee University, Seoul 02447, Korea.
Department of Science in Korean Medicine, Graduate School, Kyung Hee University, Seoul 02447, Korea.
Korean J Physiol Pharmacol. 2017 Nov;21(6):657-666. doi: 10.4196/kjpp.2017.21.6.657. Epub 2017 Oct 30.
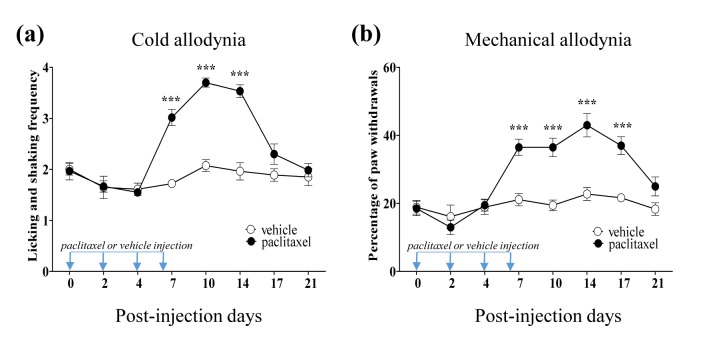
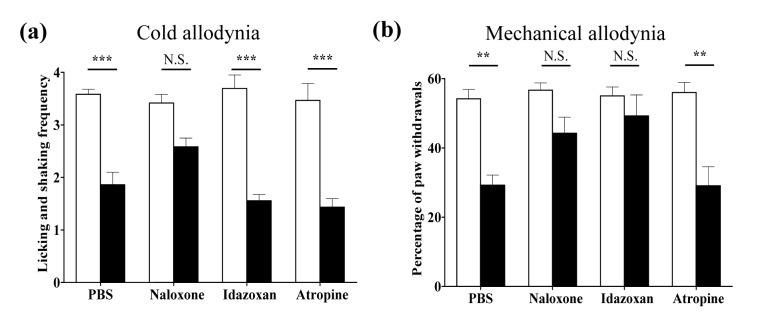
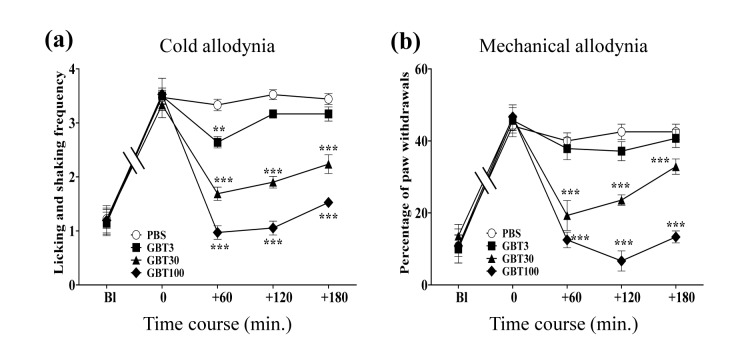
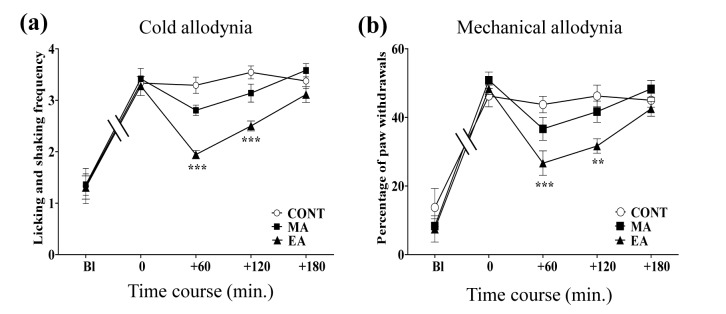
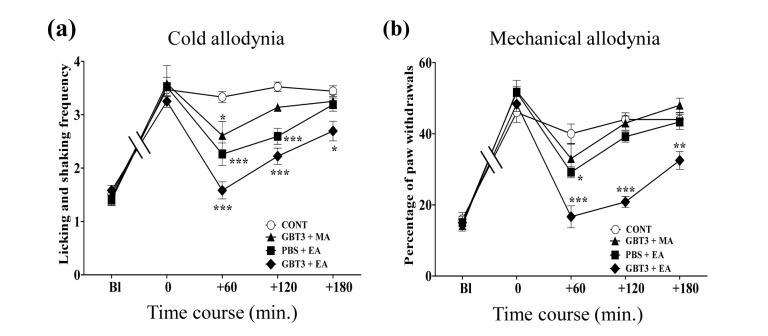
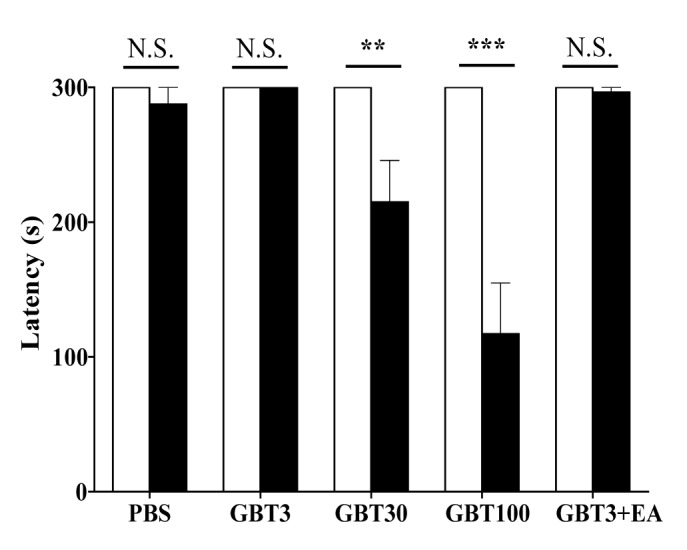
Paclitaxel, a chemotherapeutic drug, induces severe peripheral neuropathy. Gabapentin (GBT) is a first line agent used to treat neuropathic pain, and its effect is mediated by spinal noradrenergic and muscarinic cholinergic receptors. Electro-acupuncture (EA) is used for treating various types of pain via its action through spinal opioidergic and noradrenergic receptors. Here, we investigated whether combined treatment of these two agents could exert a synergistic effect on paclitaxel-induced cold and mechanical allodynia, which were assessed by the acetone drop test and von Frey filament assay, respectively. Significant signs of allodynia were observed after four paclitaxel injections (a cumulative dose of 8 mg/kg, i.p.). GBT (3, 30, and 100 mg/kg, i.p.) or EA (ST36, Zusanli) alone produced dose-dependent anti-allodynic effects. The medium and highest doses of GBT (30 and 100 mg/kg) provided a strong analgesic effect, but they induced motor dysfunction in Rota-rod tests. On the contrary, the lowest dose of GBT (3 mg/kg) did not induce motor weakness, but it provided a brief analgesic effect. The combination of the lowest dose of GBT and EA resulted in a greater and longer effect, without inducing motor dysfunction. This effect on mechanical allodynia was blocked by spinal opioidergic (naloxone, 20 μg), or noradrenergic (idazoxan, 10 μg) receptor antagonist, whereas on cold allodynia, only opioidergic receptor antagonist blocked the effect. In conclusion, the combination of the lowest dose of GBT and EA has a robust and enduring analgesic action against paclitaxel-induced neuropathic pain, and it should be considered as an alternative treatment method.
紫杉醇是一种化疗药物,可诱发严重的周围神经病变。加巴喷丁(GBT)是用于治疗神经性疼痛的一线药物,其作用是通过脊髓去甲肾上腺素能和毒蕈碱胆碱能受体介导的。电针(EA)通过其对脊髓阿片样物质能和去甲肾上腺素能受体的作用来治疗各种类型的疼痛。在此,我们研究了这两种药物联合治疗是否能对紫杉醇诱导的冷觉和机械性异常性疼痛产生协同作用,分别通过丙酮滴注试验和von Frey细丝试验进行评估。在注射四次紫杉醇(累积剂量为8 mg/kg,腹腔注射)后观察到明显的异常性疼痛迹象。单独使用GBT(3、30和100 mg/kg,腹腔注射)或EA(ST36,足三里)产生剂量依赖性的抗异常性疼痛作用。GBT的中剂量和高剂量(30和100 mg/kg)提供了较强的镇痛作用,但它们在转棒试验中诱导了运动功能障碍。相反,GBT的低剂量(3 mg/kg)未诱导运动无力,但提供了短暂的镇痛作用。低剂量的GBT与EA联合使用产生了更大且更持久的效果,且未诱导运动功能障碍。这种对机械性异常性疼痛的作用被脊髓阿片样物质能(纳洛酮,20 μg)或去甲肾上腺素能(咪唑克生,10 μg)受体拮抗剂阻断,而对于冷觉异常性疼痛,只有阿片样物质能受体拮抗剂阻断了该作用。总之,低剂量的GBT与EA联合使用对紫杉醇诱导的神经性疼痛具有强大而持久的镇痛作用,应被视为一种替代治疗方法。