Department of Cardiology, Guangdong Cardiovascular Institute, Guangdong Provincial Key Laboratory of Coronary Heart Disease Prevention, Guangdong General Hospital, Guangdong Academy of Medical Sciences, Guangzhou, Guangdong, China.
The Department of Developmental Biology, Harvard School of Dental Medicine, Harvard Medical School, Boston, MA.
J Am Heart Assoc. 2017 Dec 4;6(12):e006988. doi: 10.1161/JAHA.117.006988.
Postoperative thrombocytopenia has been reported to be correlated with adverse events, but the prognostic value of baseline thrombocytopenia is unclear. This study was undertaken to evaluate the relationship between preoperative thrombocytopenia and adverse outcomes in patients with rheumatic heart disease who underwent valve replacement surgery.
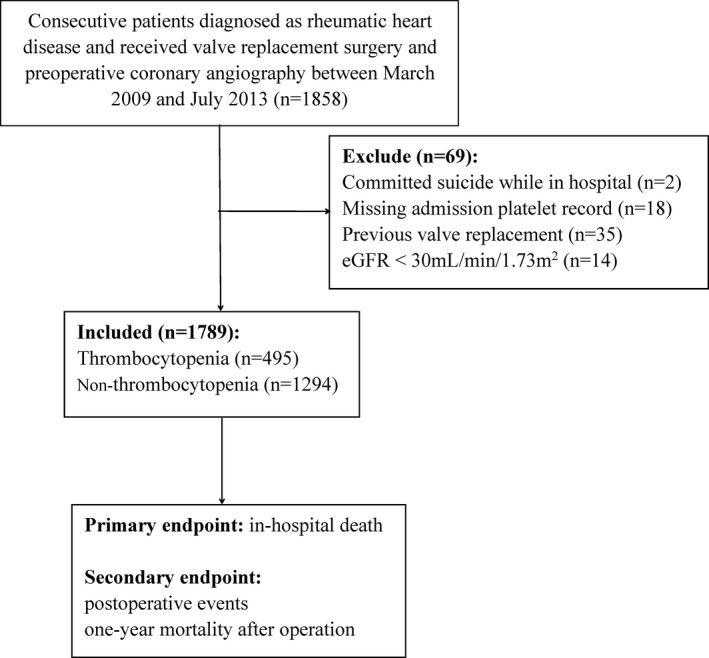
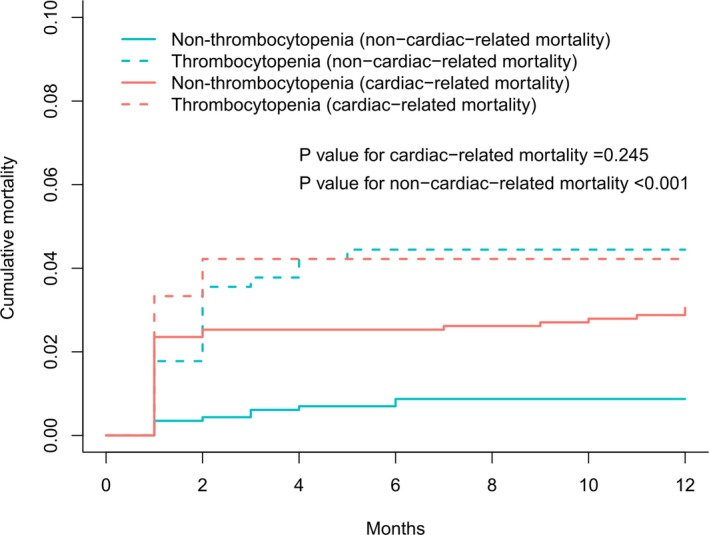
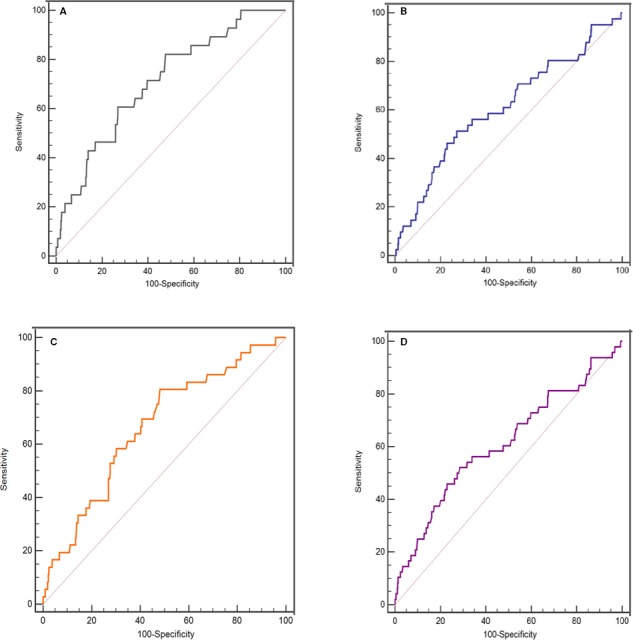
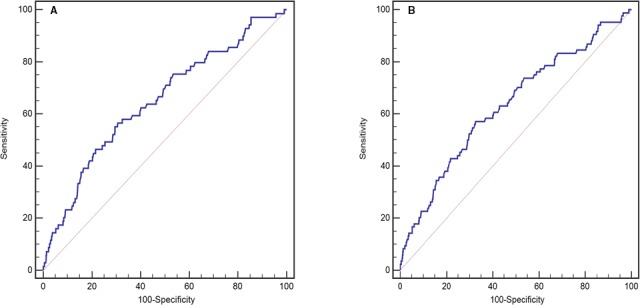
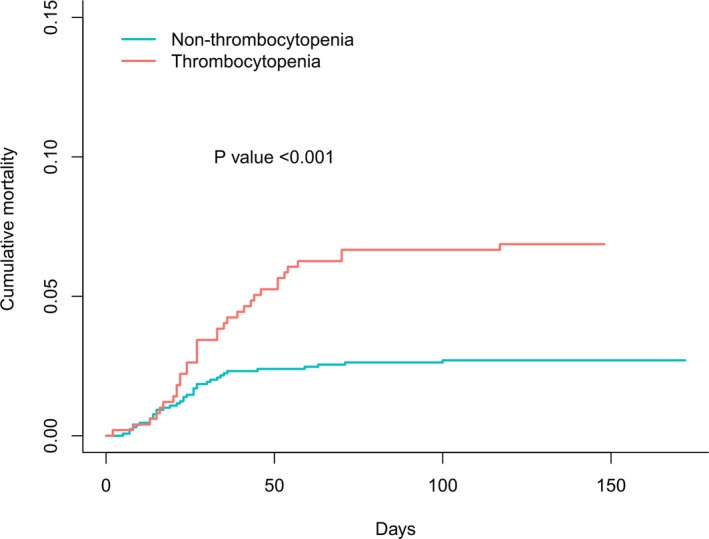
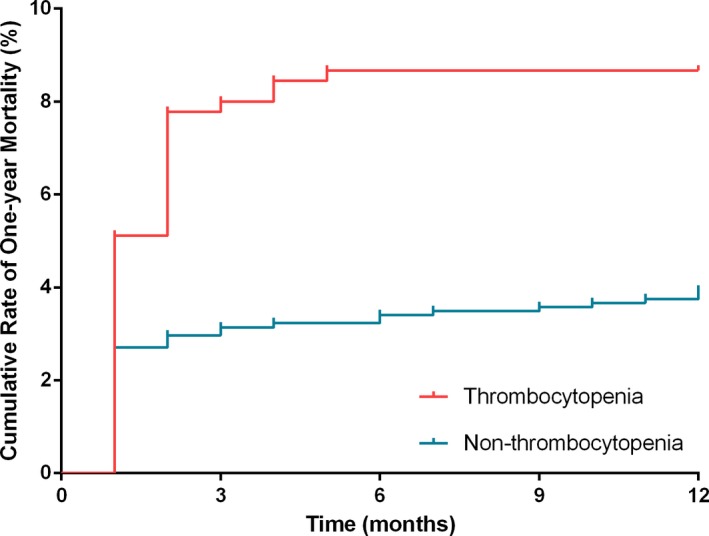
A total of 1789 patients with rheumatic heart disease undergoing valve replacement surgery were consecutively enrolled and postoperatively followed up for 1 year. Patients were stratified on the basis of presence (n=495) or absence (n=1294) of thrombocytopenia (platelet count, <150×10/L), according to hospital admission platelet counts. During the hospitalization period, 69 patients (3.9%) died. The in-hospital all-cause mortality rate was significantly higher in the thrombocytopenic group (6.9% versus 2.7%; <0.001). Multivariate analyses revealed that thrombocytopenia was independently associated with in-hospital all-cause mortality (odds ratio, 2.21; 95% confidence interval, 1.29-3.80; =0.004). Platelet counts could predict in-hospital all-cause mortality for patients both with and without previous atrial fibrillation (areas under the curve, 0.708 [<0.001] and 0.610 [=0.025], respectively). One-year survival was significantly lower in patients with thrombocytopenia compared with controls (91.3% versus 96.1%; log-rank=14.65; <0.001). In addition, thrombocytopenia was an independent predictor for postoperative 1-year all-cause mortality in multivariate Cox regression analysis.
Platelet counts, as simple and inexpensive indexes, were reliable to be used as a preoperative risk assessment tool for patients with rheumatic heart disease undergoing valve replacement surgery.
术后血小板减少与不良事件相关,但基线血小板减少的预后价值尚不清楚。本研究旨在评估风湿性心脏病患者行瓣膜置换术后术前血小板减少与不良结局的关系。
连续纳入 1789 例行瓣膜置换术的风湿性心脏病患者,并在术后随访 1 年。根据入院时血小板计数,将患者分为血小板减少(血小板计数<150×10/L)组(n=495)和血小板正常组(n=1294)。住院期间,69 例患者(3.9%)死亡。血小板减少组的住院全因死亡率明显更高(6.9%比 2.7%;<0.001)。多变量分析显示,血小板减少与住院全因死亡率独立相关(比值比,2.21;95%置信区间,1.29-3.80;=0.004)。血小板计数可预测有和无既往心房颤动患者的住院全因死亡率(曲线下面积,0.708[<0.001]和 0.610[=0.025])。与对照组相比,血小板减少患者 1 年生存率明显较低(91.3%比 96.1%;log-rank=14.65;<0.001)。此外,多变量 Cox 回归分析显示,血小板减少是术后 1 年全因死亡的独立预测因素。
血小板计数作为简单、廉价的指标,可作为风湿性心脏病患者行瓣膜置换术的术前风险评估工具。