Huang Ching-Wen, Tsai Hsiang-Lin, Yeh Yung-Sung, Su Wei-Chih, Huang Ming-Yii, Huang Chun-Ming, Chang Yu-Tang, Wang Jaw-Yuan
Graduate Institute of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan.
Division of Colorectal Surgery, Department of Surgery, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan.
BMC Surg. 2017 Dec 5;17(1):126. doi: 10.1186/s12893-017-0315-x.
The robotic system has advantages of high-definition three-dimensional vision and articular instruments with high dexterity, allowing more precise dissection in the deep and narrow pelvic cavity.
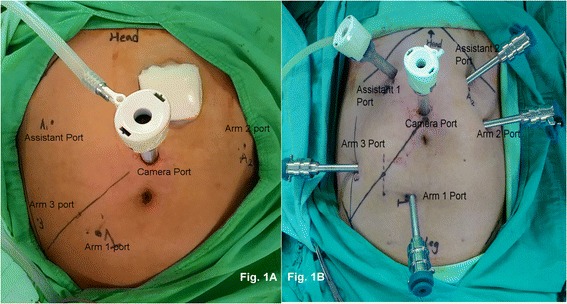
We enrolled 95 patients with stage I-III rectal cancer (adenocarcinoma) who underwent totally robotic-assisted total mesorectal excision (TME) with single-docking technique at a single institution between September 2013 and December 2016.
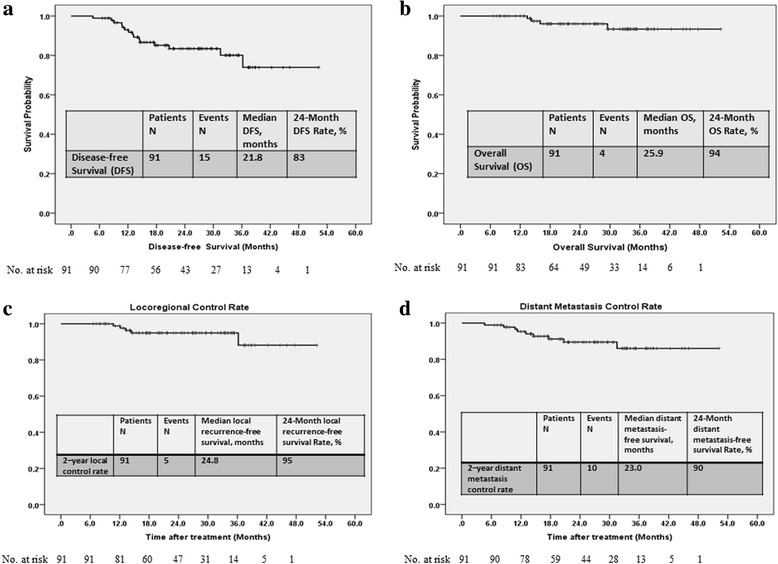
Of the 95 patients, 48 (50.5%) and 30 (31.6%) patients had lower and middle rectal cancers, respectively. Of the 75 (78.9%) patients undergoing preoperative concurrent chemoradiotherapy (CCRT), 27 (28.4%) exhibited pathologic complete response (pCR). Only four (4.2%) patients underwent abdominoperineal resection and the sphincter preservation rate was 95.8%. R0 resection was performed in 92 (96.8%) patients. Circumferential resection margin (CRM) and distal resection margin (DRM) were positive in 2 (2.1%) and 1 (1.1%) patients, respectively. The anastomotic leakage rate was 5.4% (5/95 patients). The overall complication rate was 17.9% (17/95 patients); most of them were mild. No 30-day hospital mortality occurred, and no patients required conversion to open surgery. In 92 patients undergoing R0 resection, 2-year overall survival was 94% and 2-year disease-free survival was 83%.
The results demonstrated that totally robotic-assisted TME with the single-docking technique is safe and feasible for patients with rectal cancer, with or without preoperative CCRT. Moreover, favorable pCR rate, R0 resection rate, CRM, DRM, sphincter preservation rate, and short-term oncological outcomes can be achieved by combining this approach with appropriate preoperative CCRT.
机器人系统具有高清三维视觉和高灵活性的关节器械等优势,能够在深部狭窄的盆腔内进行更精确的解剖。
我们纳入了95例I - III期直肠癌(腺癌)患者,这些患者于2013年9月至2016年12月在单一机构接受了采用单对接技术的全机器人辅助全直肠系膜切除术(TME)。
95例患者中,分别有48例(50.5%)和30例(31.6%)患有低位和中位直肠癌。在75例(78.9%)接受术前同步放化疗(CCRT)的患者中,27例(28.4%)出现病理完全缓解(pCR)。仅4例(4.2%)患者接受了腹会阴联合切除术,保肛率为95.8%。92例(96.8%)患者实现了R0切除。环周切缘(CRM)和远切缘(DRM)阳性的患者分别为2例(2.1%)和1例(1.1%)。吻合口漏率为5.4%(95例患者中的5例)。总体并发症发生率为17.9%(95例患者中的17例);大多数并发症为轻度。无30天内医院死亡病例,也无患者需要转为开放手术。在92例接受R0切除的患者中,2年总生存率为94%,2年无病生存率为83%。
结果表明,采用单对接技术的全机器人辅助TME对于直肠癌患者,无论是否接受术前CCRT,都是安全可行的。此外,通过将这种方法与适当的术前CCRT相结合,可以实现良好的pCR率、R0切除率、CRM、DRM、保肛率以及短期肿瘤学结局。