Department of Medicine, University of Toronto, Toronto, Ontario, Canada.
Division of Cardiology, St. Michael's Hospital, Toronto, Ontario, Canada.
Cancer. 2018 Mar 15;124(6):1269-1278. doi: 10.1002/cncr.31174. Epub 2017 Dec 6.
There is a paucity of information about treatment and mortality trends after acute myocardial infarction (AMI) for cancer survivors (CS).
In this population-based study, the authors compared temporal trends of treatments and outcomes (mortality, nonfatal cardiovascular outcomes), among CS and patients without cancer (the noncancer patient [NCP] group) with AMI in Ontario (Canada) using inverse probability treatment weight (IPTW)-adjusted modeling.
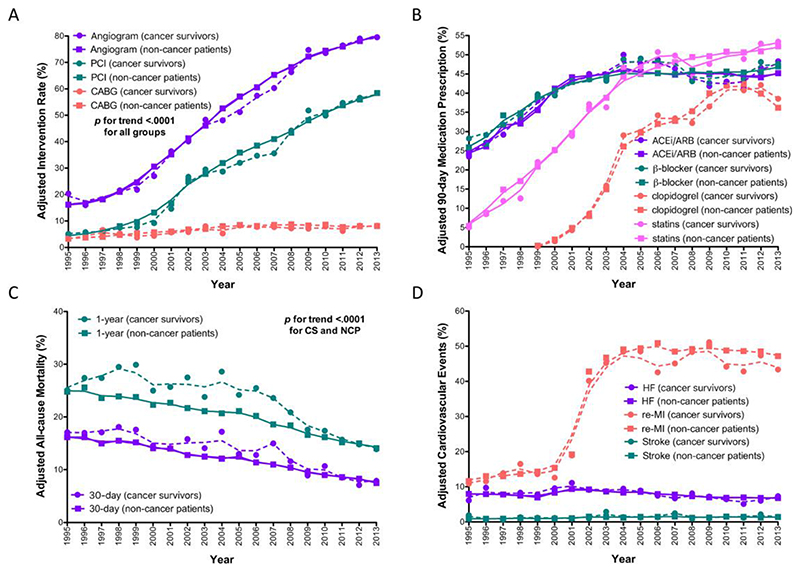
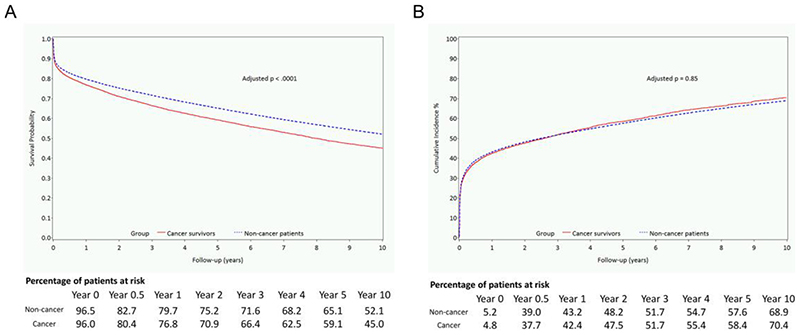
Of 270,089 patients with AMI (22,907 CS, 247,182 NCP, 1995-2013; median follow-up, 10.1 and 11.0 years, respectively), the use of invasive coronary strategies and pharmacotherapies increased and mortality declined for CS and NCP (all P < .001). At 30 days after AMI, there was no difference between CS and NCP in the receipt of coronary angiography (incidence risk ratio [IRR], 0.98; 95% confidence interval [CI], 0.96-1.01; P = .23), percutaneous coronary intervention (IRR, 0.98; 95% CI, 0.94-1.02; P = .29), or bypass (IRR, 0.93; 95% CI, 0.85-1.02; P = .11). At 90 days after AMI, there was no difference in the receipt of β-blockers, clopidogrel, or nitrates; but CS were less often prescribed angiotensin-converting enzyme inhibitors/angiotensin II receptor blockers and statins. CS had higher all-cause mortality at 30 days (adjusted hazard ratio [HR] 1.12; 95% CI, 1.07-1.17; P < .001), at 1 year (1.16; 95% CI, 1.12-1.20; P < .001), and long term (HR, 1.21; 95% CI, 1.17-1.25; P < .001) and had a greater risk of heart failure (HR, 1.08; 95% CI, 1.03-1.14; P = .001), but not myocardial re-infarction (HR, 0.98; 95% CI, 0.95-1.01; P = .22) or stroke (HR, 1.06; 95% CI, 0.97-1.16; P = .18).
Among CS and NCP with AMI in Ontario, similar improvements in mortality and receipt of treatments were observed between 1995 and 2013. However, compared with NCP, CS had a higher risk of mortality and heart failure. Cancer 2018;124:1269-78. © 2017 American Cancer Society.
癌症幸存者(CS)发生急性心肌梗死(AMI)后治疗和死亡率趋势的相关信息较为匮乏。
在这项基于人群的研究中,作者通过使用逆概率治疗加权(IPTW)调整模型,比较了安大略省(加拿大)CS 和无癌症患者(非癌症患者 [NCP] 组)的治疗和结局(死亡率、非致命性心血管结局)的时间趋势。
在 270089 例 AMI 患者(CS 22907 例,NCP 247182 例,1995-2013 年;中位随访时间分别为 10.1 和 11.0 年)中,CS 和 NCP 中侵入性冠状动脉策略和药物治疗的使用率均有所增加,死亡率均有所下降(均 P <.001)。在 AMI 后 30 天,CS 和 NCP 之间接受冠状动脉造影的情况没有差异(发生率风险比 [IRR],0.98;95%置信区间 [CI],0.96-1.01;P = .23)、经皮冠状动脉介入治疗(IRR,0.98;95% CI,0.94-1.02;P = .29)或旁路(IRR,0.93;95% CI,0.85-1.02;P = .11)。在 AMI 后 90 天,β-受体阻滞剂、氯吡格雷或硝酸盐的使用没有差异;但是 CS 较少使用血管紧张素转换酶抑制剂/血管紧张素 II 受体阻滞剂和他汀类药物。CS 在 30 天时全因死亡率更高(调整后的危险比 [HR],1.12;95% CI,1.07-1.17;P < .001),1 年时(1.16;95% CI,1.12-1.20;P < .001)和长期(HR,1.21;95% CI,1.17-1.25;P < .001),心力衰竭风险更高(HR,1.08;95% CI,1.03-1.14;P = .001),但心肌再梗死(HR,0.98;95% CI,0.95-1.01;P = .22)或中风(HR,1.06;95% CI,0.97-1.16;P = .18)的风险无差异。
在安大略省的 CS 和 NCP 中,1995 年至 2013 年间,死亡率和治疗方法的改善情况相似。然而,与 NCP 相比,CS 的死亡率和心力衰竭风险更高。癌症 2018;124:1269-78。© 2017 美国癌症协会。