Department of Research and Development, The Norwegian Air Ambulance Foundation, Drøbak.
Department of Clinical Medicine, University of Oslo.
Eur J Emerg Med. 2019 Jun;26(3):194-198. doi: 10.1097/MEJ.0000000000000529.
Cerebral revascularization in acute stroke requires robust diagnostic tools close to symptom onset. The quantitative National Institute of Health Stroke Scale (NIHSS) is widely used in-hospital, whereas shorter and less specific stroke scales are used in the prehospital field. This study explored the accuracy and potential clinical benefit of using NIHSS prehospitally.
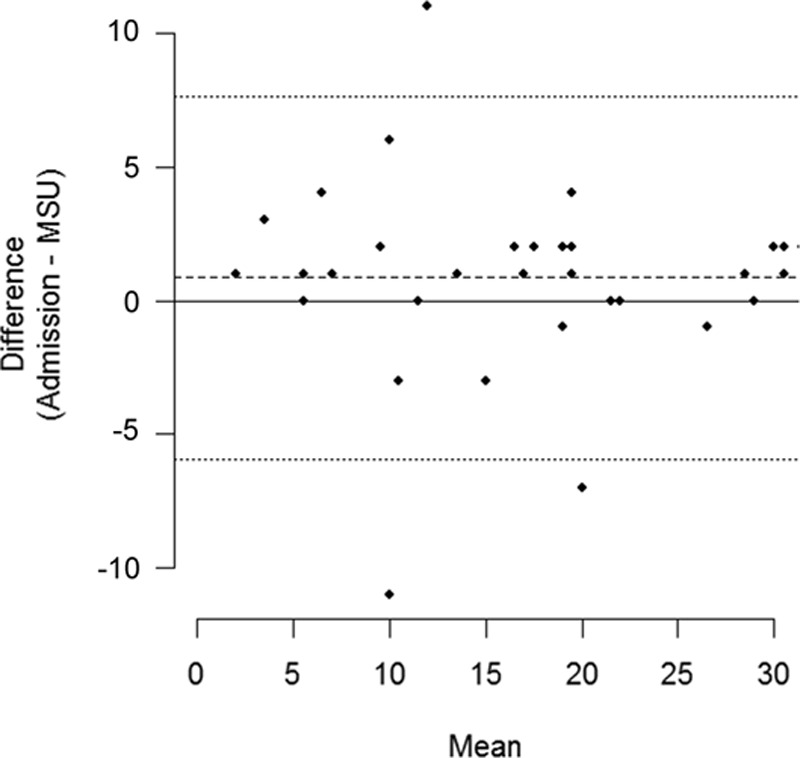
Thirteen anesthesiologists trained in prehospital critical care enrolled patients with suspected acute stroke in a mobile stroke unit. NIHSS was completed twice in the acute phase: first prehospitally and then by an on-call resident neurologist at the receiving hospital. The agreement between prehospital and in-hospital NIHSS scores was assessed by a Bland-Altman plot, and inter-rater agreement for predefined clinical categories was tested using Cohen's κ.
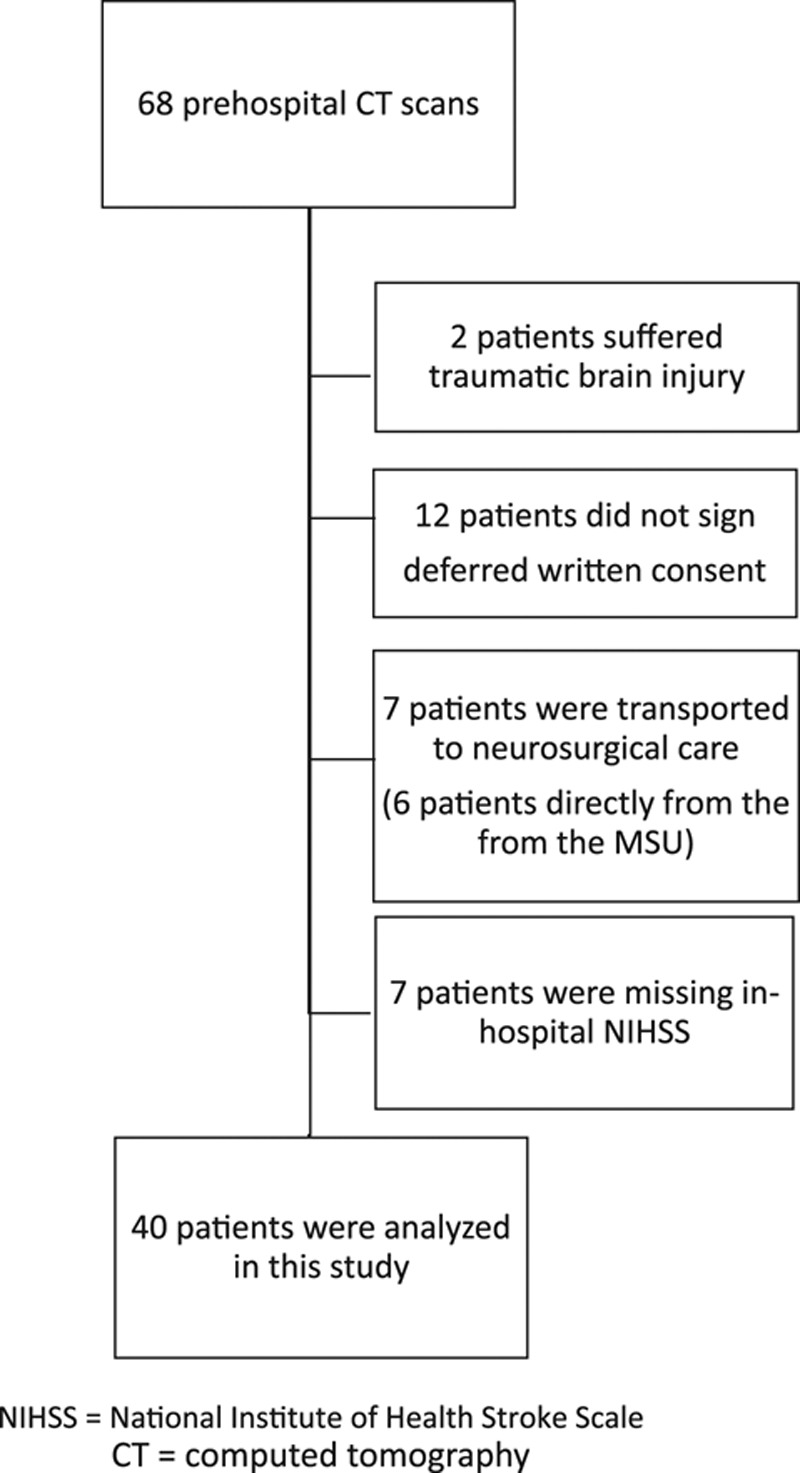
This Norwegian Acute Stroke Prehospital Project study included 40 patients for analyses. The mean numerical difference between prehospital and in-hospital NIHSS scores was 0.85, with corresponding limits of agreement from - 5.94 to 7.64. Inter-rater agreement (κ) for the corresponding clinical categories was 0.38. A prehospital diagnostic workup (NIHSS and computed tomographic examination) was completed in median (quartiles) 10 min (range: 7-14 min). Time between the prehospital and in-hospital NIHSS scores was median (quartiles) 40 min (32-48 min).
Critical care physicians in a mobile stroke unit may use the NIHSS as a clinical tool in the assessment of patients experiencing acute stroke. The disagreement in NIHSS scores was mainly for very low values and would not have changed the handling of the patients.
急性脑卒中的脑血管重建需要在症状发作时就使用强有力的诊断工具。量化的国立卫生研究院卒中量表(NIHSS)在院内广泛应用,而在院前领域则使用更短、特异性更低的卒中量表。本研究旨在探索院前使用 NIHSS 的准确性和潜在临床获益。
13 名接受过院前重症监护培训的麻醉师在移动卒中单元中招募疑似急性脑卒中的患者。NIHSS 在急性期进行了两次评估:第一次是在院前,然后由接收医院的值班神经科住院医师进行。通过 Bland-Altman 图评估院前和院内 NIHSS 评分之间的一致性,并使用 Cohen's κ 检验评估预定义临床类别之间的评分者间一致性。
挪威急性脑卒中院前项目研究共纳入了 40 例患者进行分析。院前和院内 NIHSS 评分的平均数值差异为 0.85,相应的一致性界限为-5.94 至 7.64。相应临床类别的评分者间一致性(κ)为 0.38。完成了院前诊断性检查(NIHSS 和计算机断层扫描检查)的中位数(四分位数间距)为 10 分钟(范围:7-14 分钟)。院前和院内 NIHSS 评分之间的时间中位数(四分位数间距)为 40 分钟(32-48 分钟)。
移动卒中单元的重症监护医师可以使用 NIHSS 作为评估急性脑卒中患者的临床工具。NIHSS 评分的不一致主要是因为非常低的值,而不会改变患者的处理方式。