1 Associate Professor, School of Sociology and Social Policy, University of Leeds, UK.
2 5995 Senior Lecturer, Department of Social Work, Education and Community Well Being, Northumbria University , Newcastle, UK.
J Health Serv Res Policy. 2018 Jan;23(1):57-65. doi: 10.1177/1355819617740925. Epub 2017 Dec 20.
Objectives Internationally, there has been considerable debate about the role of data in supporting quality improvement in health care. Our objective was to understand how, why and in what circumstances the feedback of aggregated patient-reported outcome measures data improved patient care. Methods We conducted a realist synthesis. We identified three main programme theories underlying the use of patient-reported outcome measures as a quality improvement strategy and expressed them as nine 'if then' propositions. We identified international evidence to test these propositions through searches of electronic databases and citation tracking, and supplemented our synthesis with evidence from similar forms of performance data. We synthesized this evidence through comparing the mechanisms and impact of patient-reported outcome measures and other performance data on quality improvement in different contexts. Results Three programme theories were identified: supporting patient choice, improving accountability and enabling providers to compare their performance with others. Relevant contextual factors were extent of public disclosure, use of financial incentives, perceived credibility of the data and the practicality of the results. Available evidence suggests that patients or their agents rarely use any published performance data when selecting a provider. The perceived motivation behind public reporting is an important determinant of how providers respond. When clinicians perceived that performance indicators were not credible but were incentivized to collect them, gaming or manipulation of data occurred. Outcome data do not provide information on the cause of poor care: providers needed to integrate and interpret patient-reported outcome measures and other outcome data in the context of other data. Lack of timeliness of performance data constrains their impact. Conclusions Although there is only limited research evidence to support some widely held theories of how aggregated patient-reported outcome measures data stimulate quality improvement, several lessons emerge from interventions sharing the same programme theories to help guide the increasing use of these measures.
在国际上,关于数据在支持医疗保健质量改进方面的作用存在相当大的争议。我们的目的是了解汇总患者报告的结果测量数据如何、为何以及在何种情况下改善患者护理。
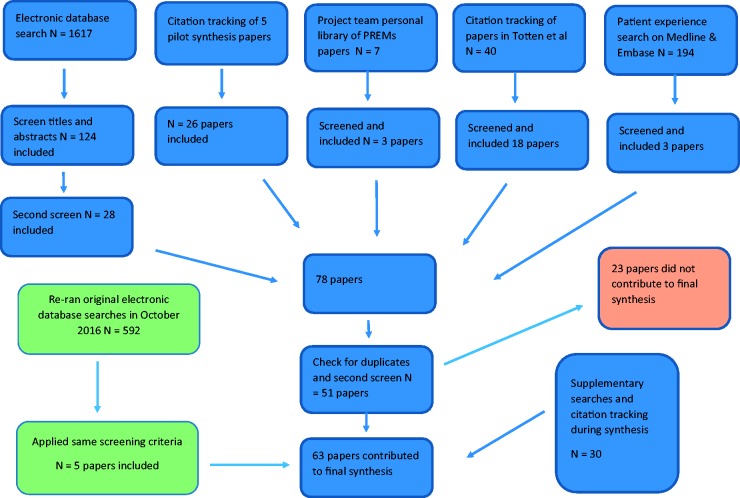
我们进行了一项实际主义综合研究。我们确定了将患者报告的结果测量作为质量改进策略的三个主要方案理论,并将其表达为九个“如果……那么”的命题。我们通过电子数据库搜索和引文追踪,确定了国际证据来检验这些命题,并通过类似形式的绩效数据补充了我们的综合证据。我们通过比较患者报告的结果测量和其他绩效数据在不同背景下对质量改进的机制和影响来综合这些证据。
确定了三个方案理论:支持患者选择、提高问责制和使提供者能够将其绩效与他人进行比较。相关的背景因素包括公开披露的程度、使用财务激励、对数据的可信度的感知以及结果的实用性。可用证据表明,患者或其代理人在选择提供者时很少使用任何发布的绩效数据。公开报告背后的感知动机是提供者如何做出反应的一个重要决定因素。当临床医生认为绩效指标不可信但因收集而受到激励时,就会出现游戏或操纵数据的情况。结果数据不能提供不良护理的原因信息:提供者需要在其他数据的背景下整合和解释患者报告的结果测量和其他结果数据。绩效数据的及时性不足限制了其影响。
尽管只有有限的研究证据支持一些关于汇总患者报告的结果测量数据如何刺激质量改进的广泛持有的理论,但从具有相同方案理论的干预措施中可以得出一些经验教训,以帮助指导这些措施的日益使用。