University Hospital Abderrahim Harouchi, Casablanca, Morocco.
Child Health Section, Glasgow University School of Medicine, Royal Hospital for Sick Children, Glasgow, UK.
Arch Dis Child. 2018 Jul;103(7):637-642. doi: 10.1136/archdischild-2017-313454. Epub 2017 Dec 21.
Thyrotoxicosis is both rarer and more severe in children than in adults, rendering management difficult and often unsatisfactory.
To ascertain outcome in a geographically defined area of Scotland between 1989 and 2014.
Retrospective case note review with follow-up questionnaire to family doctors for patients with Graves' disease and Hashimoto's thyroiditis.
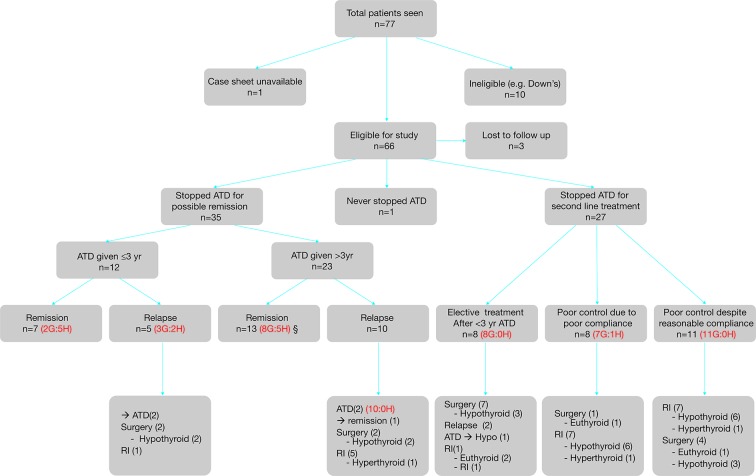
Sixty-six patients (58 females:8 males) comprising 53 with Graves' disease and 13 with Hashimoto's thyroiditis were diagnosed at median 10.4 (2.9-15.8) years and followed up for 11.8 (2.6-30.2) years. Antithyroid drug (ATD) therapy was stopped electively in 35 patients after 4.5 (1.5-8.6) years, resulting in remission in 10/13 Hashimoto's thyroiditis and 10/22 Graves' disease. Side effects occurred in 12 patients receiving carbimazole, six of whom changed to propylthiouracil; no adverse events occurred in the latter patients.Second-line therapy was given to 37 patients (34 with Graves' disease), comprising radioiodine (22) at 15.6 (9.3-24.4) years for relapse (6), poor control/adherence (14) or electively (2); and surgery (16) at 12 (6.4-21.3) years for relapse (4), poor control/adherence (5) and electively (7). Adherence problems with thyroxine replacement were reported in 10/33 patients in adulthood.
Hashimoto's thyroiditis should be distinguished from Graves' disease at diagnosis since the prognosis for remission is better. Remission rates for Graves' disease are low (10/53 patients), time to remission variable and adherence with both ATD and thyroxine replacement often problematic. We recommend (a) the giving of long-term ATD rather than a fixed course of treatment in GD and (b) meticulous and realistic counselling of families from the time of diagnosis onwards.
甲状腺功能亢进症在儿童中的发病率和严重程度均高于成人,这使得治疗变得困难,且往往效果不佳。
在苏格兰的一个特定地理区域,于 1989 年至 2014 年期间,确定甲状腺功能亢进症患者的治疗结局。
对格雷夫斯病和桥本甲状腺炎患者的病历进行回顾性病例分析,并对家庭医生进行随访问卷调查。
共纳入 66 例患者(58 例女性:8 例男性),其中 53 例患有格雷夫斯病,13 例患有桥本甲状腺炎。中位年龄为 10.4 岁(2.9-15.8 岁),随访时间为 11.8 年(2.6-30.2 年)。35 例患者在服用抗甲状腺药物(ATD)4.5 年后(1.5-8.6 年)选择停药,其中 10 例桥本甲状腺炎和 10 例格雷夫斯病患者缓解。12 例接受甲巯咪唑治疗的患者出现药物副作用,其中 6 例改用丙硫氧嘧啶;后者无不良事件发生。37 例(34 例患有格雷夫斯病)患者接受二线治疗,包括 22 例放射性碘治疗(15.6 岁,9.3-24.4 岁,原因是复发[6 例]、控制不佳/不遵医嘱[14 例]或选择[2 例])和 16 例手术治疗(12 岁,6.4-21.3 岁,原因是复发[4 例]、控制不佳/不遵医嘱[5 例]或选择[7 例])。33 例成年患者中有 10 例报告存在甲状腺素替代治疗的依从性问题。
诊断时应将桥本甲状腺炎与格雷夫斯病区分开来,因为前者的缓解预后更好。格雷夫斯病的缓解率较低(53 例患者中 10 例缓解),缓解时间不一,且对 ATD 和甲状腺素替代治疗的依从性常常存在问题。我们建议:(a)对 GD 患者长期给予 ATD 而非固定疗程的治疗;(b)从诊断开始,对患者及其家属进行细致和现实的指导。