Department of Radiation Oncology, Inselspital, Bern University Hospital, University of Bern, Freiburgstrasse 15, 3010, Bern, Switzerland.
Department of Radiation Oncology, Kantonsspital, St. Gallen, Switzerland.
Radiat Oncol. 2017 Dec 22;12(1):202. doi: 10.1186/s13014-017-0938-1.
Cisplatin and gemcitabine combined with conventional radiation therapy in the treatment of cervical cancer patients results in a favorable outcome but with excess toxicity. The purpose of this study was to evaluate the toxicity profile of dual chemotherapy and highly conformal external beam radiotherapy with image guided adaptive brachytherapy.
Seventeen patients with cervical carcinoma FIGO stage IB2-IIIB were treated with curative intent between 2011 and 2015. A total dose of 50.4 Gy was prescribed to the elective pelvic nodal volume. Patients with FDG-PET/CT positive lymph nodes (n = 15; 83.3%) received an additional boost to a total dose of 62 Gy. Chemotherapy prescription goals were: concomitant during 5 weeks of external beam radiotherapy (EBRT) 40 mg/m2 cisplatin and 125 mg/m gemcitabine, followed by adjuvant chemotherapy from week 10 (2 cycles 50 mg/m cisplatin and 1000 mg/m gemcitabine). EBRT was followed by 3-4 fractions (6 Gy per fraction) of intrauterine image guided adaptive brachytherapy. Toxicities were graded according to the common terminology criteria for adverse events (CTCAE v 4.0).
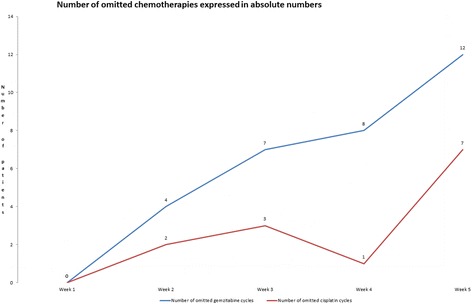
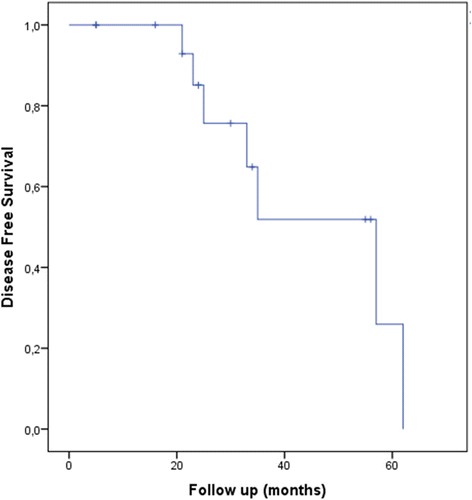
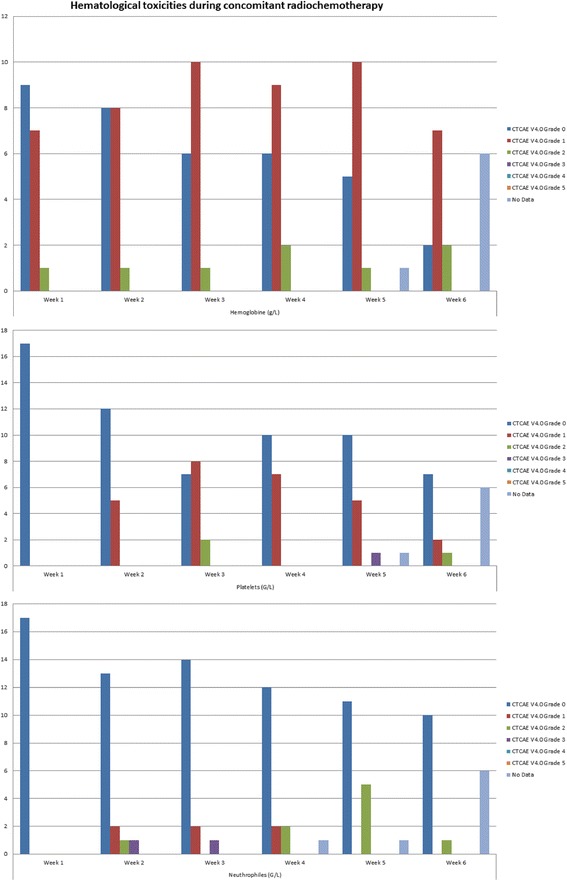
One (6%) patient developed acute grade 3 diarrhea. We did not record any other acute or late gastrointestinal or urogenital toxicity higher that grade 3. Most common acute hematological toxicity was anemia grade 2 recorded in 10 (59%) patients. There was only one case of grade 3 neutropenia (6%). The number of patients that received the complete chemotherapy regimen was gradually declining during the course of therapy. From week 2 to 5, gemcitabine was omitted in 4 (24%),7 (41%), 8 (47%), and 12 (71%) patients respectively, similarly, cisplatin was omitted in 2 (12%),3 (18%),1 (6%) and 7 (41%) patients respectively. Adjuvant chemotherapy was omitted in 8 patients (47%). During a median follow-up time of 20 months (5 to 63 months) 6 (35%) patients developed disease relapse with 5 (29%) of them in the form of systemic disease.
In contrast to previous findings cisplatin and gemcitabine in combination with highly conformal radiation therapy seems to have an acceptable toxicity profile. Further studies are needed to determine the optimal dosage of the proposed therapy concept.
顺铂和吉西他滨联合常规放射治疗宫颈癌患者可获得良好的疗效,但毒性较大。本研究旨在评估双重化疗和图像引导自适应近距离放射治疗联合高适形外照射治疗的毒性谱。
17 例FIGO 分期 IB2-IIIB 期宫颈癌患者于 2011 年至 2015 年接受根治性治疗。计划盆腔淋巴结区域总剂量为 50.4Gy。15 例(83.3%)FDG-PET/CT 阳性淋巴结患者给予总剂量 62Gy 的额外加量。化疗处方目标为:外照射放疗(EBRT)5 周期间同时给予 40mg/m2 顺铂和 125mg/m2 吉西他滨,然后从第 10 周开始辅助化疗(2 个周期 50mg/m2 顺铂和 1000mg/m2 吉西他滨)。EBRT 后行 3-4 次宫腔内图像引导自适应近距离放疗(每分次 6Gy)。毒性分级采用不良事件常用术语标准(CTCAE v 4.0)。
1 例(6%)患者发生急性 3 级腹泻。我们没有记录任何其他急性或晚期胃肠道或泌尿生殖系统毒性高于 3 级。最常见的急性血液学毒性是 10 例(59%)患者的 2 级贫血。仅有 1 例(6%)中性粒细胞减少症 3 级。接受完整化疗方案的患者人数在治疗过程中逐渐减少。从第 2 周到第 5 周,分别有 4 例(24%)、7 例(41%)、8 例(47%)和 12 例(71%)患者分别遗漏吉西他滨,同样有 2 例(12%)、3 例(18%)、1 例(6%)和 7 例(41%)患者分别遗漏顺铂。8 例(47%)患者未接受辅助化疗。中位随访时间为 20 个月(5-63 个月),6 例(35%)患者出现疾病复发,其中 5 例(29%)为全身疾病。
与以往发现相比,顺铂和吉西他滨联合高适形放疗似乎具有可接受的毒性谱。需要进一步研究确定该治疗方案的最佳剂量。