Kido Koji, Ito Hiroyuki, Yamamoto Yudai, Makita Koshi, Uchida Tokujiro
Department of Anesthesiology, Tokyo Medical and Dental University, Graduate School of Medical and Dental Sciences, 1-5-45 Yushima, Bunkyo-ku, Tokyo, 113-8519, Japan.
Division of Anesthesia, Kyoundo Hospital, Tokyo, Japan.
J Anesth. 2018 Feb;32(1):120-131. doi: 10.1007/s00540-017-2441-0. Epub 2017 Dec 29.
Propofol infusion syndrome (PRIS) is a lethal condition caused by propofol overdose. Previous studies suggest that pathophysiological mechanisms underlying PRIS involve mitochondrial dysfunction; however, these mechanisms have not been fully elucidated. This study aimed to establish an experimental model of propofol-induced cytotoxicity using cultured human induced pluripotent stem cell (iPSC)-derived cardiomyocytes to determine the mechanisms behind propofol-induced mitochondrial dysfunction, and to evaluate the protective effects of coenzyme Q10 (CoQ10).
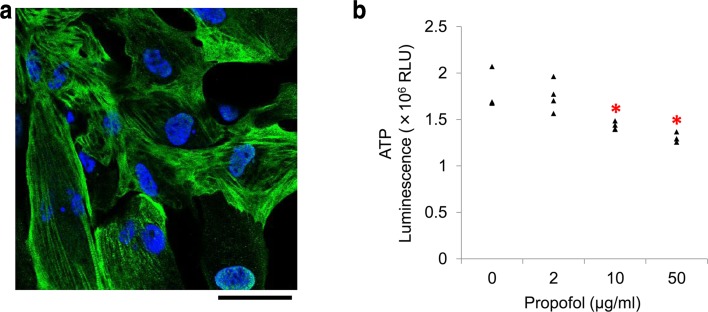
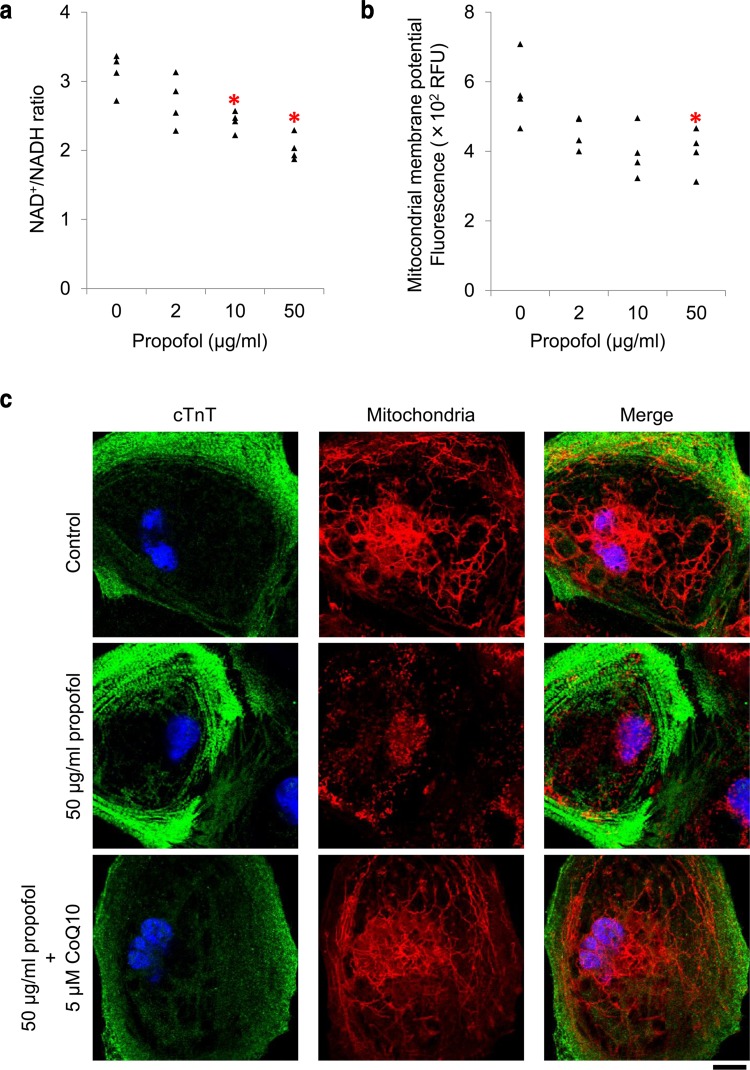
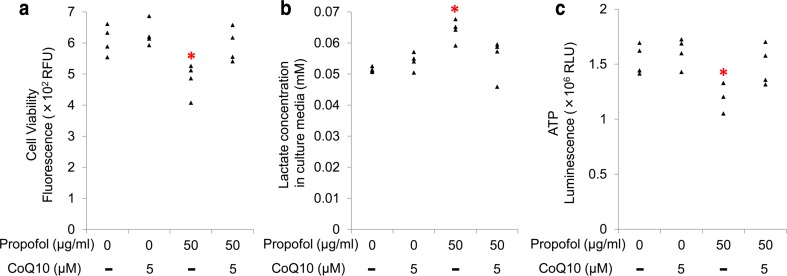
Human iPSC-derived cardiomyocytes were exposed to propofol (0, 2, 10, or 50 µg/ml) with or without 5 µM CoQ10. Mitochondrial function was assessed by measuring intracellular ATP, lactate concentrations in culture media, NAD/NADH ratio, and the mitochondrial membrane potential. Propofol-induced cytotoxicity was evaluated by analysis of cell viability. Expression levels of genes associated with mitochondrial energy metabolism were determined by PCR. Intracellular morphological changes were analyzed by confocal microscopy.
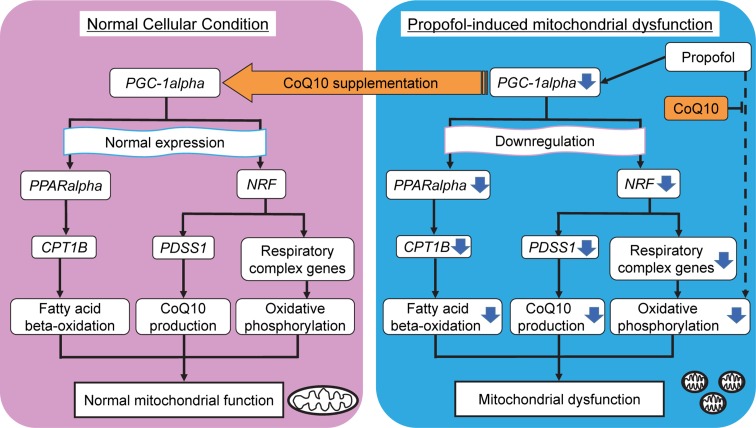
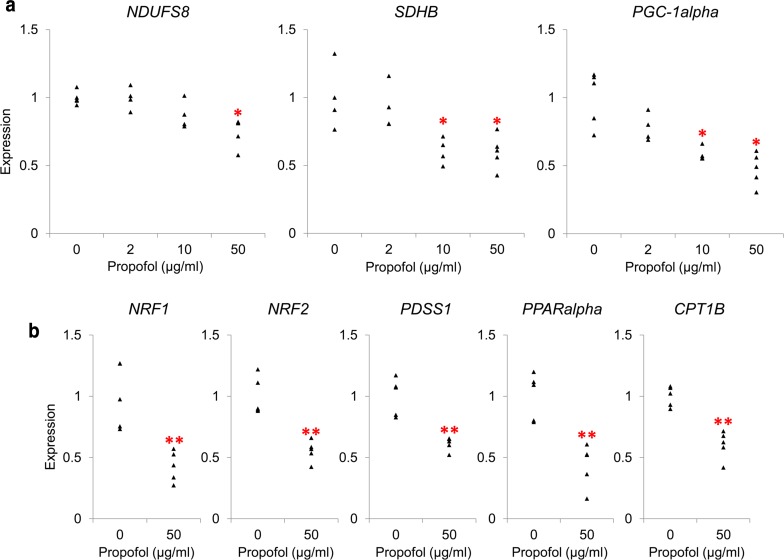
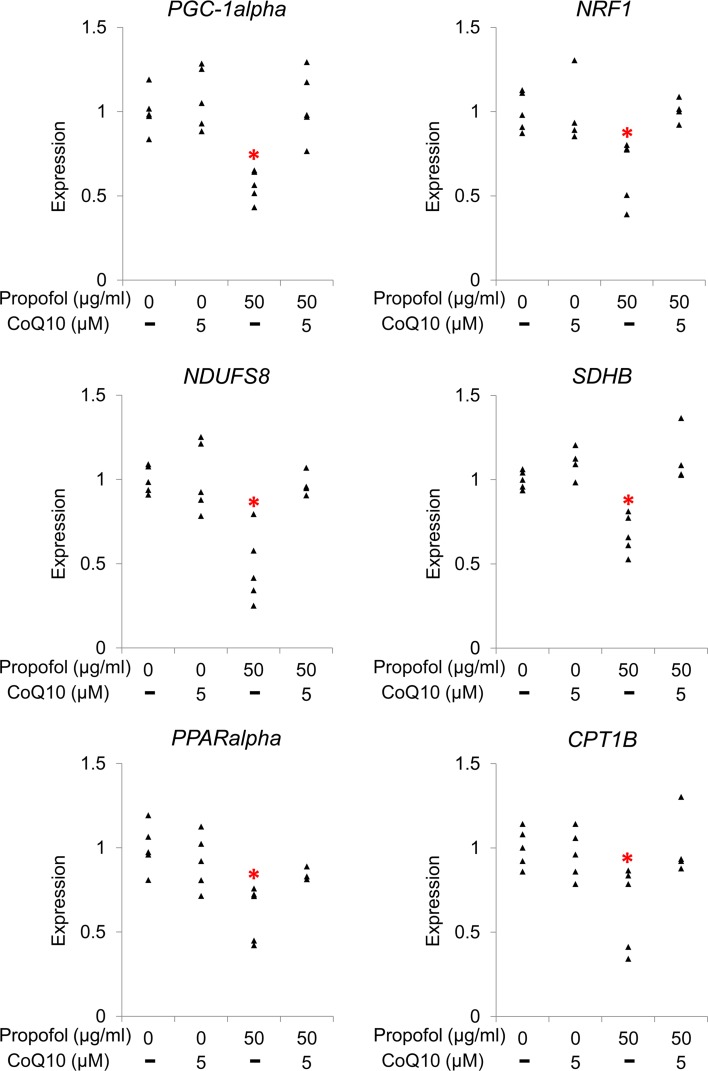
Treatment with 50 µg/ml propofol for 48 h reduced cell viability. High concentrations of propofol (≥ 10 µg/ml) induced mitochondrial dysfunction accompanied by downregulation of gene expression of PGC-1alpha and its downstream targets (NDUFS8 and SDHB, which are involved in the respiratory chain reaction; and CPT1B, which regulates beta-oxidation). Cardiomyocytes co-treated with 5 µM CoQ10 exhibited resistance to propofol-induced toxicity through recovery of gene expression.
Propofol-induced cytotoxicity in human iPSC-derived cardiomyocytes may be associated with mitochondrial dysfunction via downregulation of PGC-1alpha-regulated genes associated with mitochondrial energy metabolism. Co-treatment with CoQ10 protected cardiomyocytes from propofol-induced cytotoxicity.
丙泊酚输注综合征(PRIS)是一种由丙泊酚过量引起的致死性疾病。先前的研究表明,PRIS的病理生理机制涉及线粒体功能障碍;然而,这些机制尚未完全阐明。本研究旨在利用培养的人诱导多能干细胞(iPSC)来源的心肌细胞建立丙泊酚诱导的细胞毒性实验模型,以确定丙泊酚诱导线粒体功能障碍的机制,并评估辅酶Q10(CoQ10)的保护作用。
将人iPSC来源的心肌细胞暴露于含或不含5 μM CoQ10的丙泊酚(0、2、10或50 μg/ml)中。通过测量细胞内ATP、培养基中的乳酸浓度、NAD/NADH比值和线粒体膜电位来评估线粒体功能。通过分析细胞活力评估丙泊酚诱导的细胞毒性。通过PCR测定与线粒体能量代谢相关基因的表达水平。通过共聚焦显微镜分析细胞内形态变化。
用50 μg/ml丙泊酚处理48小时可降低细胞活力。高浓度丙泊酚(≥10 μg/ml)诱导线粒体功能障碍,同时伴有PGC-1α及其下游靶点(参与呼吸链反应的NDUFS8和SDHB;以及调节β氧化的CPT1B)基因表达下调。与5 μM CoQ10共同处理的心肌细胞通过基因表达的恢复表现出对丙泊酚诱导毒性的抗性。
丙泊酚诱导的人iPSC来源心肌细胞的细胞毒性可能通过下调与线粒体能量代谢相关的PGC-1α调节基因与线粒体功能障碍有关。与CoQ10共同处理可保护心肌细胞免受丙泊酚诱导的细胞毒性。