Begg Gordon A, Karim Rashed, Oesterlein Tobias, Graham Lee N, Hogarth Andrew J, Page Stephen P, Pepper Christopher B, Rhode Kawal, Lip Gregory Y H, Holden Arun V, Plein Sven, Tayebjee Muzahir H
Department of Cardiology, Leeds General Infirmary, Leeds, United Kingdom.
Leeds Institute of Cardiovascular and Metabolic Medicine, University of Leeds, Leeds, United Kingdom.
PLoS One. 2018 Jan 2;13(1):e0189936. doi: 10.1371/journal.pone.0189936. eCollection 2018.
To test the ability of four circulating biomarkers of fibrosis, and of low left atrial voltage, to predict recurrence of atrial fibrillation after catheter ablation.
Circulating biomarkers potentially may be used to improve patient selection for atrial fibrillation ablation. Low voltage areas in the left atrium predict arrhythmia recurrence when mapped in sinus rhythm. This study tested type III procollagen N terminal peptide (PIIINP), galectin-3 (gal-3), fibroblast growth factor 23 (FGF-23), and type I collagen C terminal telopeptide (ICTP), and whether low voltage areas in the left atrium predicted atrial fibrillation recurrence, irrespective of the rhythm during mapping.
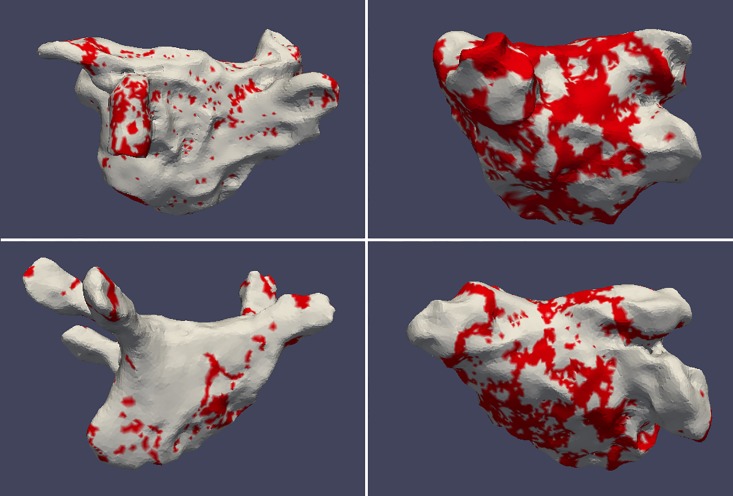
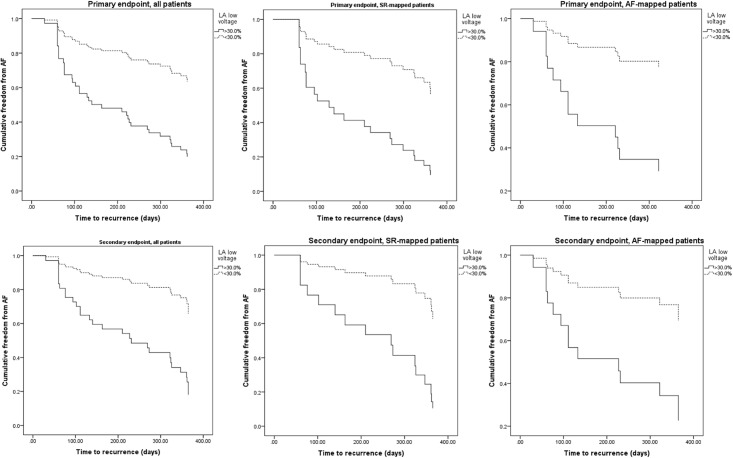
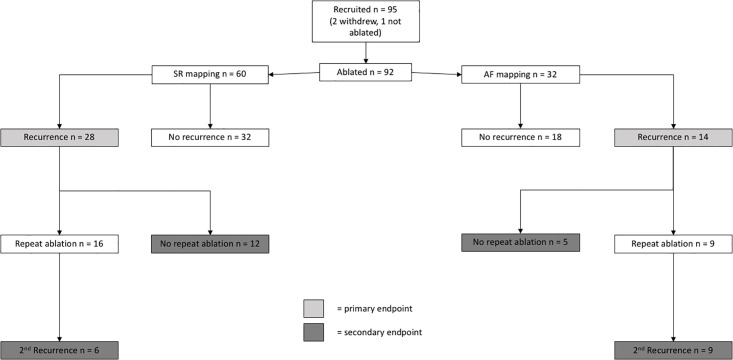
92 atrial fibrillation ablation patients were studied. Biomarker levels in peripheral and intra-cardiac blood were measured with enzyme-linked immunosorbent assay. Low voltage (<0.5mV) was expressed as a proportion of the mapped left atrial surface area. Follow-up was one year. The primary endpoint was recurrence of arrhythmia. The secondary endpoint was a composite of recurrence despite two procedures, or after one procedure if no second procedure was undertaken.
The biomarkers were not predictive of either endpoint. After multivariate Cox regression analysis, high proportion of low voltage area in the left atrium was found to predict the primary endpoint in sinus rhythm mapping (hazard ratio 4.323, 95% confidence interval 1.337-13.982, p = 0.014) and atrial fibrillation mapping (hazard ratio 5.195, 95% confidence interval 1.032-26.141, p = 0.046). This effect was also apparent for the secondary endpoint.
The studied biomarkers do not predict arrhythmia recurrence after catheter ablation. Left atrial voltage is an independent predictor of recurrence, whether the left atrium is mapped in atrial fibrillation or sinus rhythm.
检测四种纤维化循环生物标志物以及低左房电压预测导管消融术后房颤复发的能力。
循环生物标志物可能有助于改善房颤消融患者的选择。左房低电压区域在窦性心律下进行标测时可预测心律失常复发。本研究检测了III型前胶原N端肽(PIIINP)、半乳糖凝集素-3(gal-3)、成纤维细胞生长因子23(FGF-23)和I型胶原C端肽(ICTP),以及左房低电压区域是否能预测房颤复发,而不考虑标测时的心律。
对92例房颤消融患者进行研究。采用酶联免疫吸附测定法测量外周血和心内血中的生物标志物水平。低电压(<0.5mV)以标测的左房表面积的比例表示。随访1年。主要终点为心律失常复发。次要终点为尽管进行了两次手术仍复发,或如果未进行第二次手术则在一次手术后复发的综合情况。
这些生物标志物均不能预测任何一个终点。多变量Cox回归分析后发现,左房低电压区域比例高可预测窦性心律标测时的主要终点(风险比4.323,95%置信区间1.337 - 13.982,p = 0.014)和房颤标测时的主要终点(风险比5.195,95%置信区间1.032 - 26.141,p = 0.046)。该效应在次要终点中也很明显。
所研究的生物标志物不能预测导管消融术后心律失常复发。无论左房在房颤还是窦性心律下进行标测,左房电压都是复发的独立预测因素。