Uryu Kumiko, Nishimura Riki, Kataoka Keisuke, Sato Yusuke, Nakazawa Atsuko, Suzuki Hiromichi, Yoshida Kenichi, Seki Masafumi, Hiwatari Mitsuteru, Isobe Tomoya, Shiraishi Yuichi, Chiba Kenichi, Tanaka Hiroko, Miyano Satoru, Koh Katsuyoshi, Hanada Ryoji, Oka Akira, Hayashi Yasuhide, Ohira Miki, Kamijo Takehiko, Nagase Hiroki, Takimoto Tetsuya, Tajiri Tatsuro, Nakagawara Akira, Ogawa Seishi, Takita Junko
Department of Pediatrics, Graduate School of Medicine, The University of Tokyo, Tokyo, Japan.
Department of Pathology and Tumor Biology, Graduate School of Medicine, University of Kyoto, Kyoto, Japan.
Oncotarget. 2017 Nov 18;8(64):107513-107529. doi: 10.18632/oncotarget.22495. eCollection 2017 Dec 8.
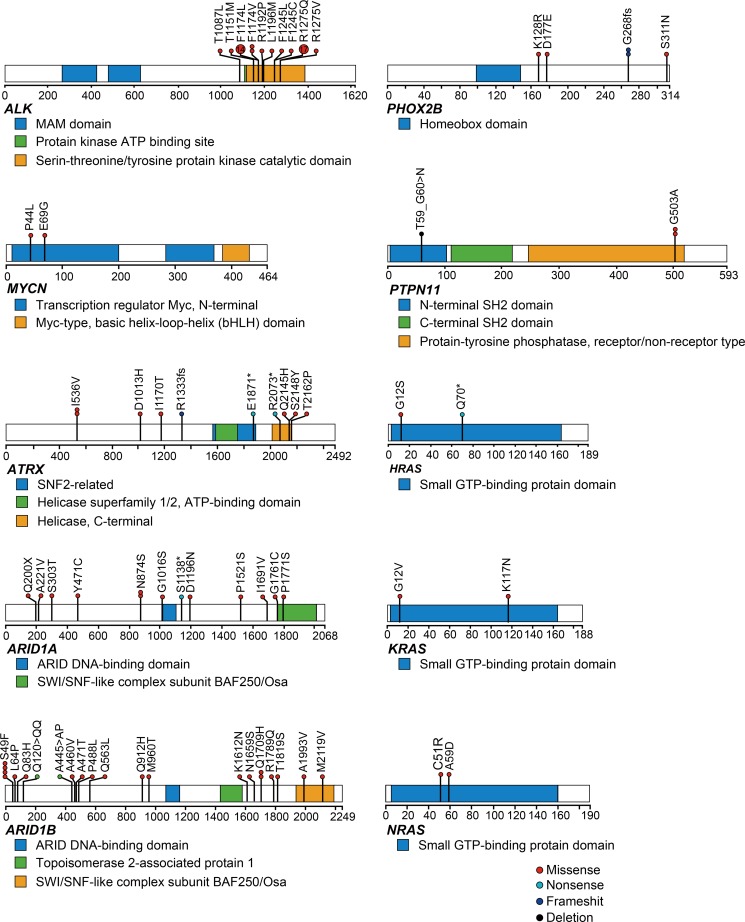
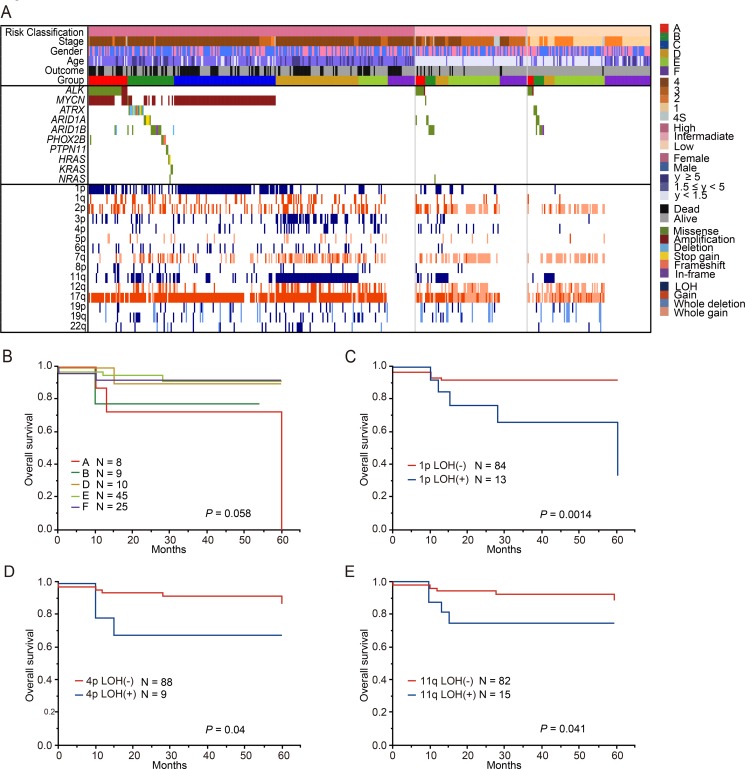
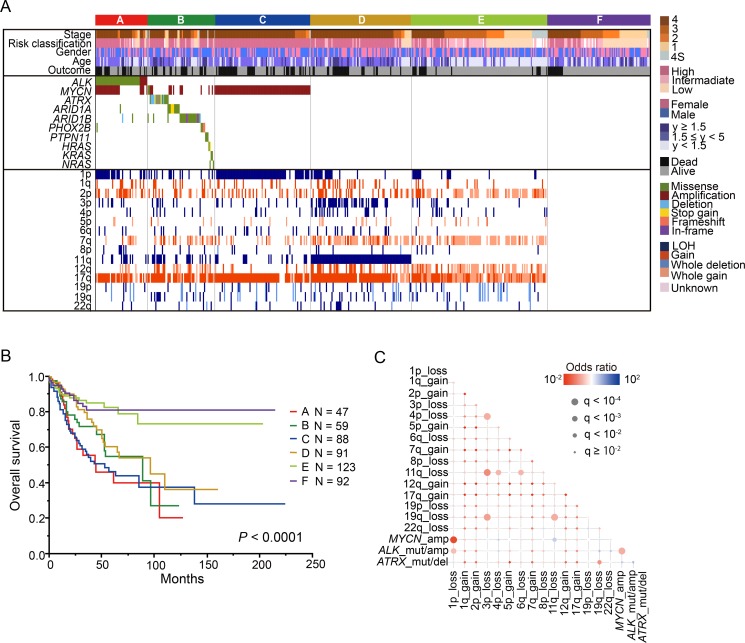
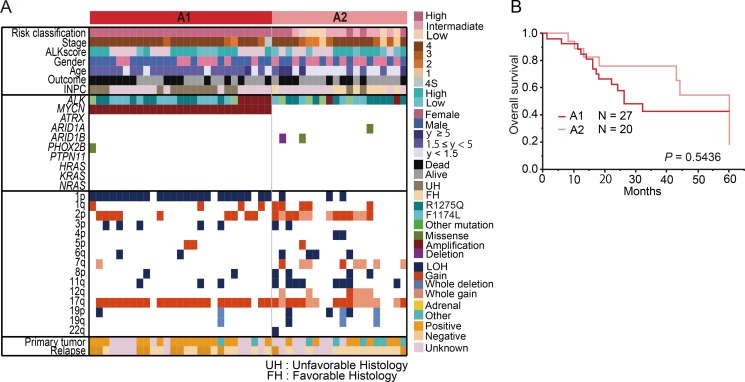
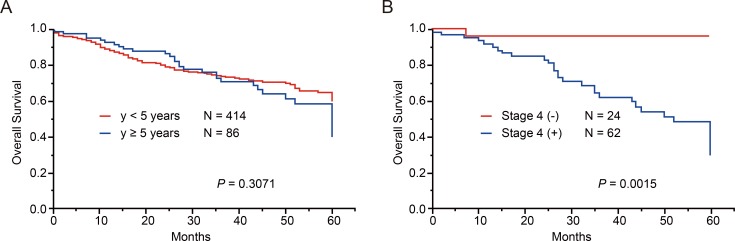
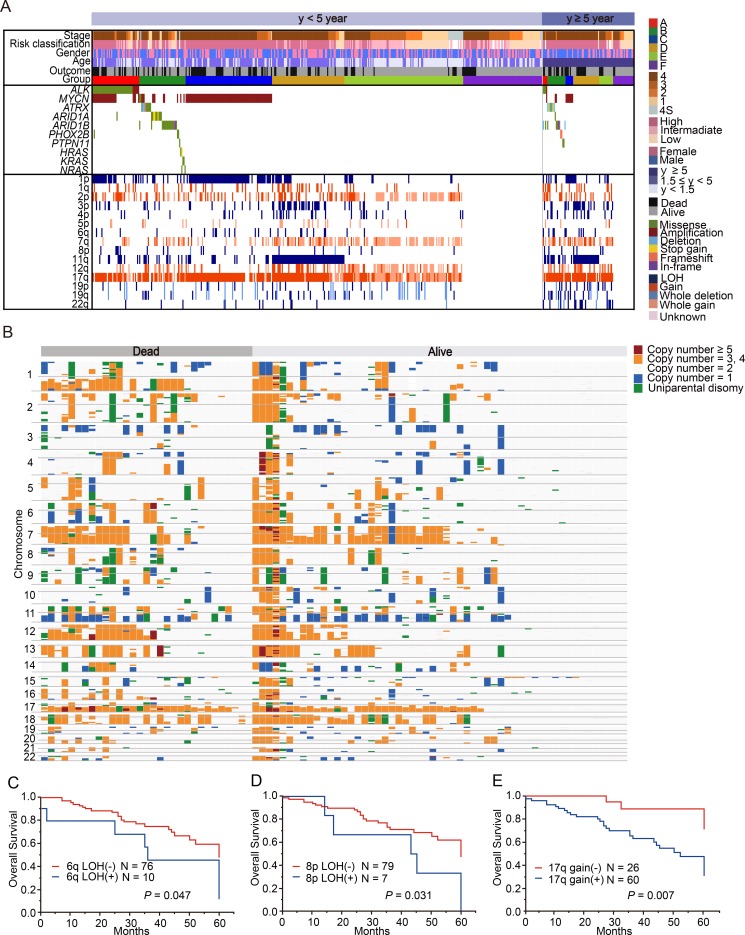
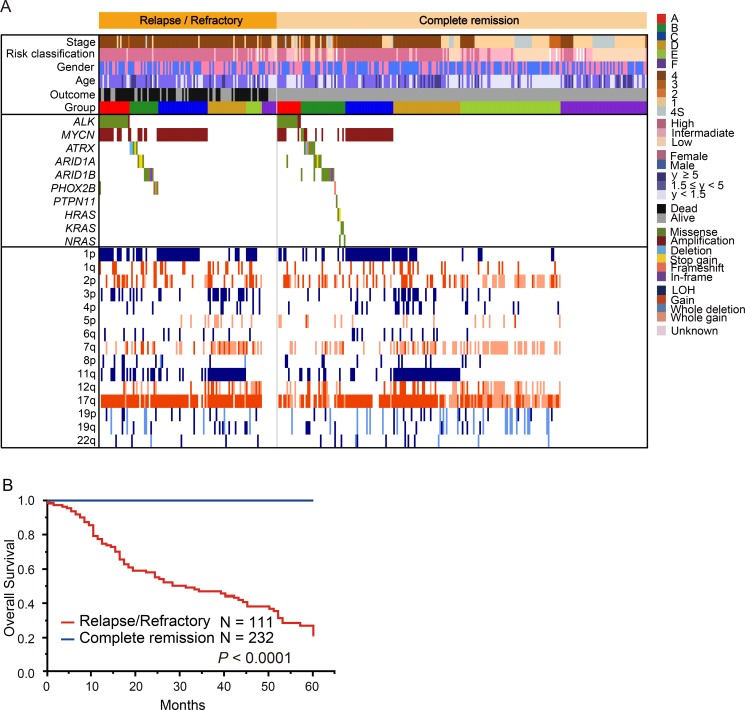
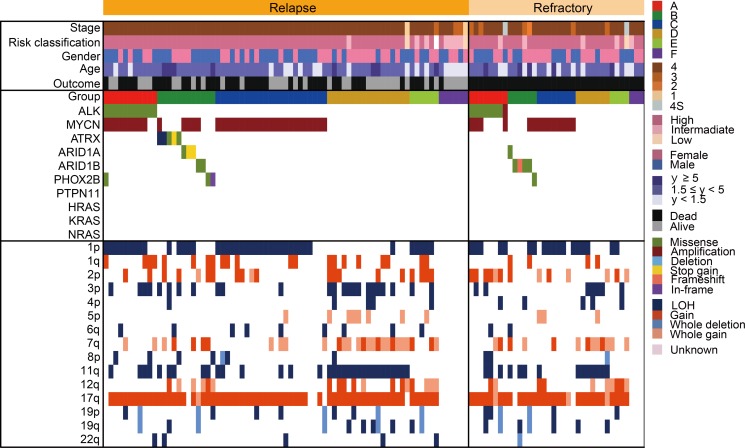
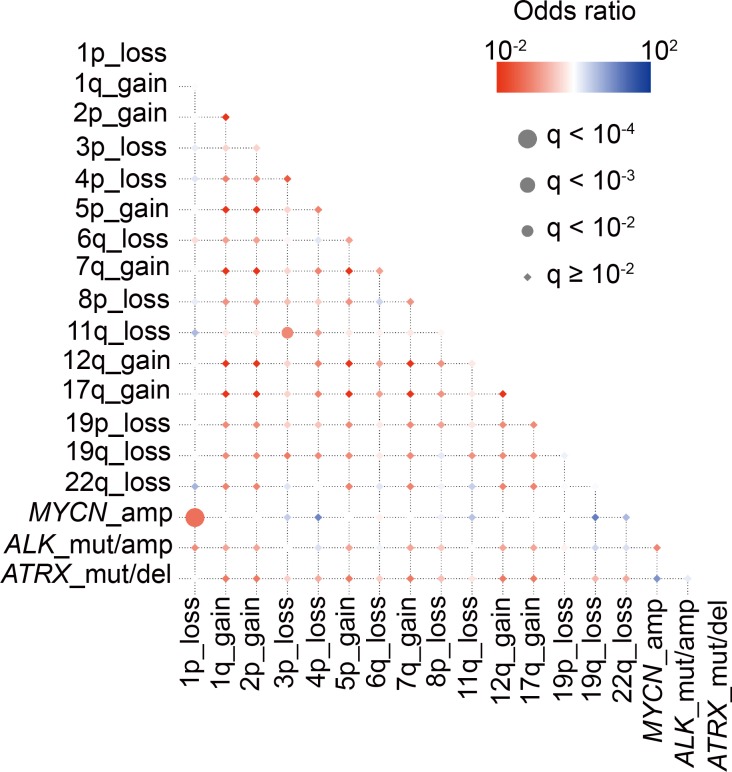
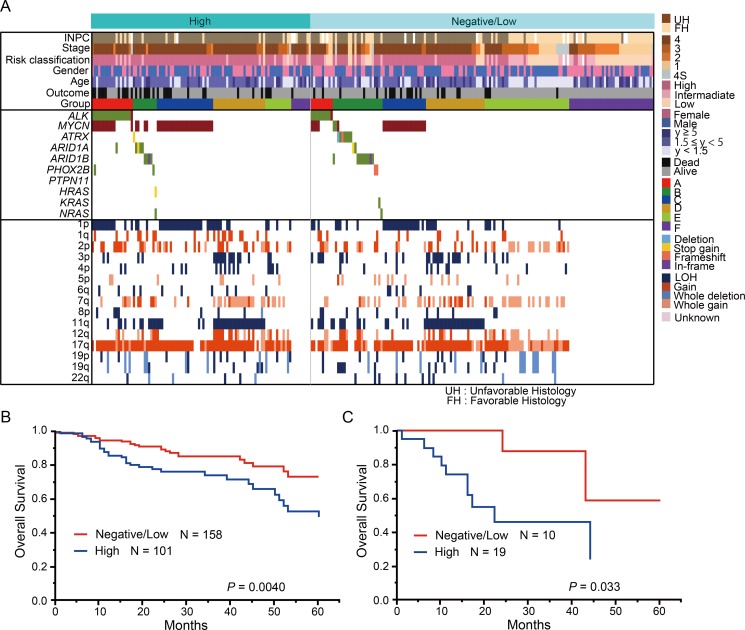
To provide better insight into the genetic signatures of neuroblastomas, we analyzed 500 neuroblastomas (included specimens from JNBSG) using targeted-deep sequencing for 10 neuroblastoma-related genes and SNP arrays analysis. ALK expression was evaluated using immunohistochemical analysis in 259 samples. Based on genetic alterations, the following 6 subgroups were identified: groups A ( abnormalities), B (other gene mutations), C ( amplification), D (11q loss of heterozygosity [LOH]), E (at least 1 copy number variants), and F (no genetic changes). Groups A to D showed advanced disease and poor prognosis, whereas groups E and F showed excellent prognosis. Intriguingly, in group A, amplification was not a significant prognostic marker, while high ALK expression was a relevant indicator for prognosis ( = 0.033). Notably, the co-existence of amplification and 1p LOH, and the co-deletion of 3p and 11q were significant predictors of relapse ( = 0.043 and = 0.040). Additionally, 6q/8p LOH and 17q gain were promising indicators of survival in patients older than 5 years, and 1p, 4p, and 11q LOH potentially contributed to outcome prediction in the intermediate-risk group. Our genetic overview clarifies the clinical impact of genetic signatures and aids in the better understanding of genetic basis of neuroblastoma.
为了更深入地了解神经母细胞瘤的基因特征,我们使用针对10个神经母细胞瘤相关基因的靶向深度测序和单核苷酸多态性(SNP)阵列分析,对500例神经母细胞瘤(包括来自JNBSG的标本)进行了分析。在259个样本中,使用免疫组织化学分析评估ALK表达。基于基因改变,确定了以下6个亚组:A组(异常)、B组(其他基因突变)、C组(扩增)、D组(11号染色体杂合性缺失[LOH])、E组(至少1个拷贝数变异)和F组(无基因改变)。A至D组显示疾病进展且预后不良,而E组和F组显示预后良好。有趣的是,在A组中,扩增不是一个显著的预后标志物,而高ALK表达是一个相关的预后指标(P = 0.033)。值得注意的是,扩增与1p LOH同时存在,以及3p和11q同时缺失是复发的显著预测指标(P = 0.043和P = 0.040)。此外,6q/8p LOH和17q增益是5岁以上患者生存的有希望的指标,1p、4p和11q LOH可能有助于中危组的预后预测。我们的基因概述阐明了基因特征的临床影响,并有助于更好地理解神经母细胞瘤的遗传基础。