Department of Internal Medicine, Section on Cardiology, Wake Forest School of Medicine, Winston Salem, North Carolina.
Epidemiological Cardiology Research Center, Department of Epidemiology and Prevention, Wake Forest School of Medicine, Winston-Salem, North Carolina.
J Am Coll Cardiol. 2018 Jan 2;71(1):1-8. doi: 10.1016/j.jacc.2017.10.071.
Although silent myocardial infarction (SMI) accounts for about one-half of the total number of myocardial infarctions (MIs), the risk of heart failure (HF) among patients with SMI is not well established.
The purpose of this study was to examine the association of SMI and clinically manifested myocardial infarction (CMI) with HF, as compared with patients with no MI.
This analysis included 9,243 participants from the ARIC (Atherosclerosis Risk In Communities) study who were free of cardiovascular disease at baseline (ARIC visit 1: 1987 to 1989). SMI was defined as electrocardiographic evidence of MI without CMI after the baseline until ARIC visit 4 (1996 to 1998). HF events were ascertained starting from ARIC visit 4 until 2010 in individuals free of HF before that visit.
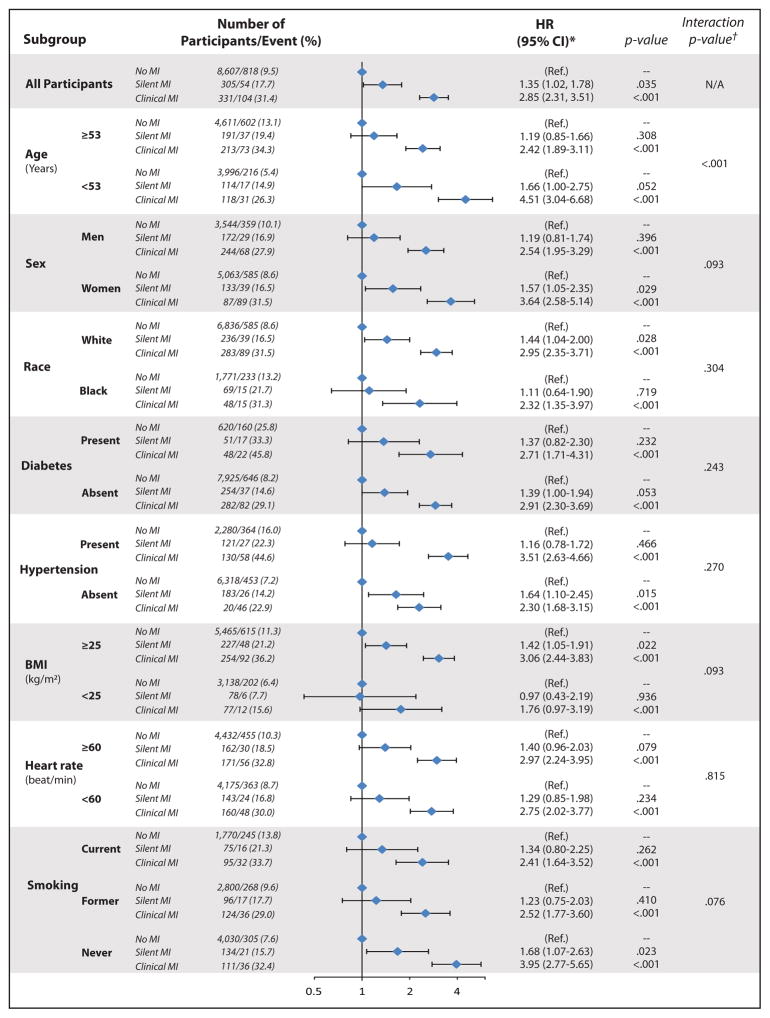
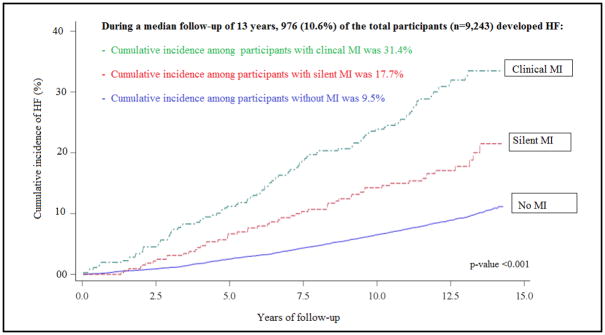
Between ARIC visits 1 and 4, 305 SMIs and 331 CMIs occurred. After ARIC visit 4 and during a median follow-up of 13.0 years, 976 HF events occurred. The incidence rate of HF was higher in both CMI and SMI participants than in those without MI (incidence rates per 1,000 person-years were 30.4, 16.2, and 7.8, respectively; p < 0.001). In a model adjusted for demographics and HF risk factors, both SMI (hazard ratio [HR]: 1.35; 95% confidence interval [CI]: 1.02 to 1.78) and CMI (HR: 2.85; 95% CI: 2.31 to 3.51) were associated with increased risk of HF compared with no MI. These associations were consistent in subgroups of participants stratified by several HF risk predictors. However, the risk of HF associated with SMI was stronger in those younger than the median age (53 years) (HR: 1.66; 95% CI: 1.00 to 2.75 vs. HR: 1.19; 95% CI: 0.85 to 1.66, respectively; overall interaction p by MI type <0.001).
SMI is associated with an increased risk of HF. Future research is needed to examine the cost effectiveness of screening for SMI as part of HF risk assessment, and to identify preventive therapies to improve the risk of HF among patients with SMI.
尽管无症状性心肌梗死(SMI)约占心肌梗死(MI)总数的一半,但 SMI 患者发生心力衰竭(HF)的风险尚不清楚。
本研究旨在探讨 SMI 和有临床表现的心肌梗死(CMI)与 HF 的关系,并与无 MI 的患者进行比较。
本分析纳入了 ARIC(社区动脉粥样硬化风险)研究中的 9243 名参与者,他们在基线时(ARIC 访视 1:1987 年至 1989 年)无心血管疾病。SMI 的定义为基线后至 ARIC 访视 4(1996 年至 1998 年)期间出现心电图提示 MI 但无 CMI。HF 事件从 ARIC 访视 4 开始,直至 2010 年,在该访视之前无 HF 的个体中进行确定。
在 ARIC 访视 1 和 4 之间,发生了 305 例 SMI 和 331 例 CMI。在 ARIC 访视 4 之后和中位随访 13.0 年期间,发生了 976 例 HF 事件。CMI 和 SMI 患者的 HF 发生率均高于无 MI 患者(每 1000 人年的发生率分别为 30.4、16.2 和 7.8,p<0.001)。在调整人口统计学和 HF 危险因素的模型中,SMI(危险比[HR]:1.35;95%置信区间[CI]:1.02 至 1.78)和 CMI(HR:2.85;95% CI:2.31 至 3.51)与 HF 风险增加相关与无 MI 相比。这些关联在按几个 HF 风险预测因素分层的参与者亚组中是一致的。然而,在年龄中位数(53 岁)以下的参与者中,与 SMI 相关的 HF 风险更高(HR:1.66;95% CI:1.00 至 2.75 与 HR:1.19;95% CI:0.85 至 1.66,总体交互作用 p<0.001)。
SMI 与 HF 风险增加相关。需要进一步研究筛查 SMI 作为 HF 风险评估一部分的成本效益,并确定预防治疗方法,以改善 SMI 患者的 HF 风险。