Stankiewicz Karita Helen C, Moss Nicholas J, Laschansky Ellen, Drolette Linda, Magaret Amalia S, Selke Stacey, Gardella Carolyn, Wald Anna
Department of Medicine, University of Washington, Seattle.
Division of Communicable Disease Control and Prevention, Alameda County Public Health Department, Oakland, California.
Open Forum Infect Dis. 2017 Nov 6;4(4):ofx248. doi: 10.1093/ofid/ofx248. eCollection 2017 Fall.
Neonatal herpes is a potentially devastating infection that results from acquisition of herpes simplex virus (HSV) type 1 or 2 from the maternal genital tract at the time of vaginal delivery. Current guidelines recommend (1) cesarean delivery if maternal genital HSV lesions are present at the time of labor and (2) antiviral suppressive therapy for women with known genital herpes to decrease HSV shedding from the genital tract at the time of vaginal delivery. However, most neonatal infections occur in infants born to women without a history of genital HSV, making current prevention efforts ineffective for this group. Although routine serologic HSV testing of women during pregnancy could identify women at higher risk of intrapartum viral shedding, it is uncertain how this knowledge might impact intrapartum management, and a potential concern is a higher rate of cesarean sections among women known to be HSV-2 seropositive.
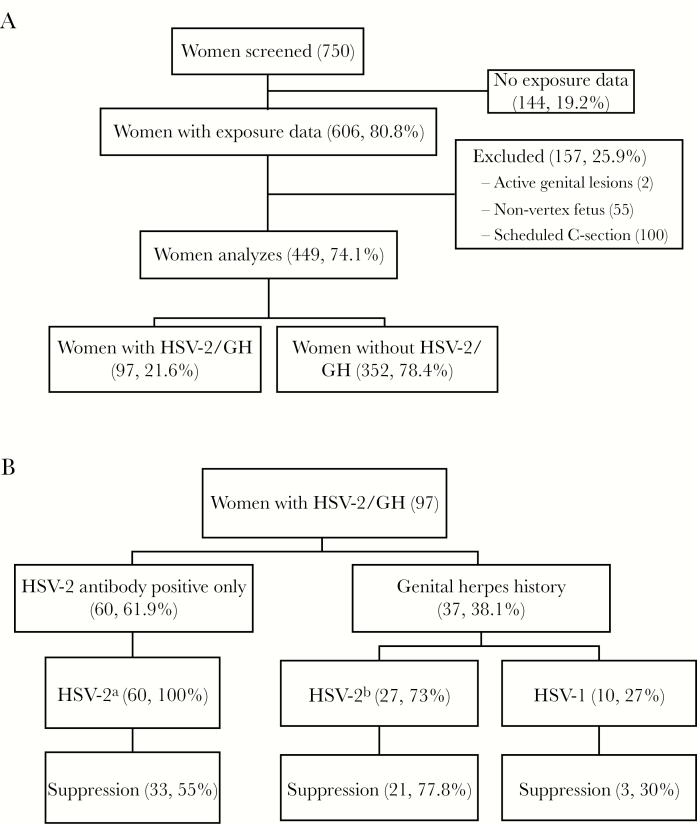
To assess the effects of prenatal HSV-2 antibody testing, history of genital herpes, and use of suppressive antiviral medication on the intrapartum management of women, we investigated the frequency of invasive obstetric procedures and cesarean deliveries. We conducted a retrospective cohort study of pregnant women delivering at the University of Washington Medical center in Seattle, Washington. We defined the exposure of interest as HSV-2 antibody positivity or known history of genital herpes noted in prenatal records. The primary outcome was intrapartum procedures including fetal scalp electrode, artificial rupture of membranes, intrauterine pressure catheter, or operative vaginal delivery (vacuum or forceps). The secondary outcome was incidence of cesarean birth. Univariate and multivariable logistic regressions were performed.
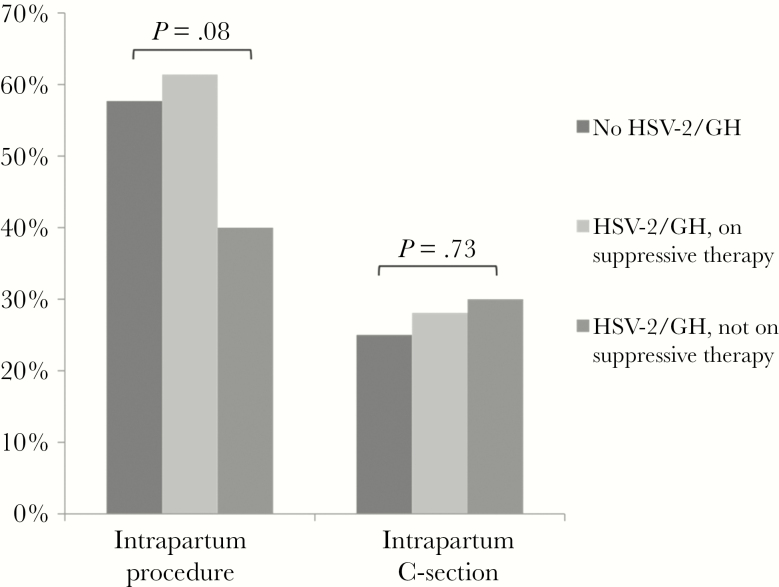
From a total of 449 women included in the analysis, 97 (21.6%) were HSV-2 seropositive or had a history of genital herpes (HSV-2/GH). Herpes simplex virus-2/GH women not using suppressive antiviral therapy were less likely to undergo intrapartum procedures than women without HSV-2/GH (odds ratio [OR], 0.49; 95% confidence interval [CI], 0.25-0.95; = .036), but this relationship was attenuated after adjustment for potential confounders (adjusted OR, 0.69; 95% CI, 0.34-1.41; = .31). There was no difference in intrapartum procedures for women on suppressive therapy versus women without HSV-2/GH (OR, 1.17; 95% CI, 0.66-2.07; = .60). Similar proportions of cesarean sections were performed within each group of women: 25% without history of HSV-2/GH, 30% on suppressive treatment, and 28.1% without suppressive treatment (global, = .73).
In this single-site study, provider awareness of genital herpes infection either by HSV serotesting or history was associated with fewer invasive obstetric procedures shown to be associated with neonatal herpes, but it was not associated with an increased rate of cesarean birth.
新生儿疱疹是一种潜在的毁灭性感染,它是在阴道分娩时由母体生殖道感染1型或2型单纯疱疹病毒(HSV)所致。当前指南建议:(1)如果分娩时母体生殖道存在HSV病变,则行剖宫产;(2)对已知有生殖器疱疹的女性进行抗病毒抑制治疗,以减少阴道分娩时生殖道HSV的排出。然而,大多数新生儿感染发生在无生殖器HSV病史的女性所生的婴儿中,这使得当前的预防措施对该群体无效。虽然孕期对女性进行常规HSV血清学检测可识别出分娩时病毒排出风险较高的女性,但尚不确定这一信息如何影响分娩期管理,且一个潜在问题是已知HSV-2血清学阳性的女性剖宫产率较高。
为评估产前HSV-2抗体检测、生殖器疱疹病史以及使用抗病毒抑制药物对女性分娩期管理的影响,我们调查了侵入性产科操作和剖宫产的频率。我们对在华盛顿州西雅图市华盛顿大学医学中心分娩的孕妇进行了一项回顾性队列研究。我们将感兴趣的暴露因素定义为产前记录中HSV-2抗体阳性或已知生殖器疱疹病史。主要结局是分娩期操作,包括胎儿头皮电极、人工破膜、宫内压力导管或阴道助产(真空吸引或产钳助产)。次要结局是剖宫产发生率。进行了单因素和多因素逻辑回归分析。
在纳入分析的449名女性中,97名(21.6%)为HSV-2血清学阳性或有生殖器疱疹病史(HSV-2/ GH)。未使用抗病毒抑制治疗的HSV-2/ GH女性比无HSV-2/ GH的女性进行分娩期操作的可能性更小(优势比[OR],0.49;95%置信区间[CI],0.25 - 0.95;P = 0.036),但在对潜在混杂因素进行校正后,这种关系减弱(校正后OR,0.69;95% CI,0.34 - 1.41;P = 0.31)。接受抑制治疗的女性与无HSV-2/ GH的女性在分娩期操作方面没有差异(OR,1.17;95% CI,0.66 - 2.07;P = 0.60)。每组女性的剖宫产比例相似:无HSV-2/ GH病史的女性为25%,接受抑制治疗的女性为30%,未接受抑制治疗的女性为28.1%(总体,P = 0.73)。
在这项单中心研究中,通过HSV血清学检测或病史提高医护人员对生殖器疱疹感染的认识,与较少的被证明与新生儿疱疹相关的侵入性产科操作有关,但与剖宫产率增加无关。