Department of Endocrinology, Academic Medical Centre, University of Amsterdam, Postbus 22660, 1100 DD, Amsterdam, the Netherlands.
The George Institute for Global Health, University of Sydney, Sydney, NSW, Australia.
Diabetologia. 2018 Apr;61(4):780-789. doi: 10.1007/s00125-017-4539-1. Epub 2018 Jan 8.
AIMS/HYPOTHESIS: Previous studies have suggested that the haemoglobin glycation index (HGI) can be used as a predictor of diabetes-related complications in individuals with type 1 and type 2 diabetes. We investigated whether HGI was a predictor of adverse outcomes of intensive glucose lowering and of diabetes-related complications in general, using data from the Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) trial.
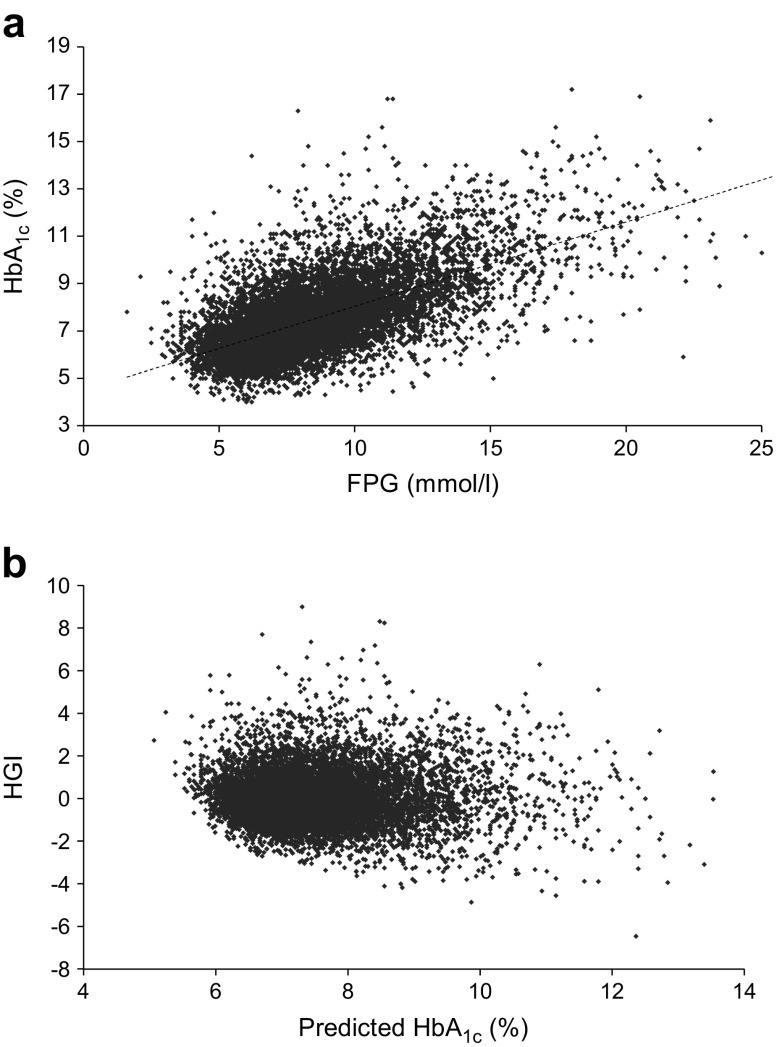
We studied participants in the ADVANCE trial with data available for baseline HbA and fasting plasma glucose (FPG) (n = 11,083). HGI is the difference between observed HbA and HbA predicted from a simple linear regression of HbA on FPG. Using Cox regression, we investigated the association between HGI, both categorised and continuous, and adverse outcomes, considering treatment allocation (intensive or standard glucose control) and compared prediction of HGI and HbA.
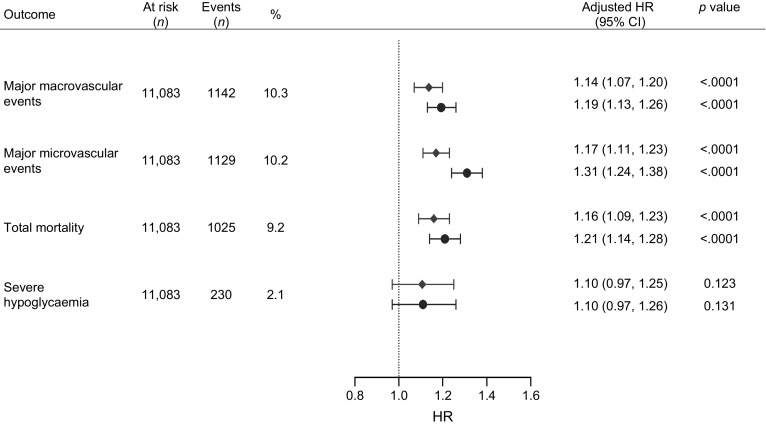
Intensive glucose control lowered mortality risk in individuals with high HGI only (HR 0.74 [95% CI 0.61, 0.91]; p = 0.003), while there was no difference in the effect of intensive treatment on mortality in those with high HbA. Irrespective of treatment allocation, every SD increase in HGI was associated with a significant risk increase of 14-17% for macrovascular and microvascular disease and mortality. However, when adjusted for identical covariates, HbA was a stronger predictor of these outcomes than HGI.
CONCLUSIONS/INTERPRETATION: HGI predicts risk for complications in ADVANCE participants, irrespective of treatment allocation, but no better than HbA. Individuals with high HGI have a lower risk for mortality when on intensive treatment. Given the discordant results and uncertain relevance beyond HbA, clinical use of HGI in type 2 diabetes cannot currently be recommended.
目的/假设:先前的研究表明,血红蛋白糖化指数(HGI)可用于预测 1 型和 2 型糖尿病患者的糖尿病相关并发症。我们利用来自糖尿病和血管疾病行动:培哚普利和二甲双胍缓释片控制评估(ADVANCE)试验的数据,研究了 HGI 是否可以预测强化血糖降低的不良结局和一般的糖尿病相关并发症。
我们研究了 ADVANCE 试验中具有基线 HbA 和空腹血浆葡萄糖(FPG)数据的参与者(n=11083)。HGI 是观察到的 HbA 与通过 HbA 与 FPG 的简单线性回归预测的 HbA 之间的差异。使用 Cox 回归,我们研究了 HGI (分类和连续)与不良结局之间的关联,同时考虑了治疗分配(强化或标准血糖控制),并比较了 HGI 和 HbA 的预测能力。
只有高 HGI 的个体接受强化血糖控制可降低死亡率风险(HR 0.74 [95%CI 0.61, 0.91];p=0.003),而高 HbA 的个体接受强化治疗对死亡率的影响则无差异。无论治疗分配如何,HGI 每增加一个标准差,大血管和微血管疾病及死亡率的风险都会显著增加 14-17%。然而,当调整相同的协变量时,HbA 是这些结局的更强预测因子,优于 HGI。
结论/解释:HGI 预测 ADVANCE 参与者的并发症风险,与治疗分配无关,但不如 HbA 好。接受强化治疗的高 HGI 个体的死亡率风险较低。鉴于不一致的结果和不确定的 HbA 以外的相关性,目前不能推荐在 2 型糖尿病中使用 HGI。