Kantar Health, New York, NY, USA.
Sanofi US, Inc., Bridgewater, NJ, USA.
Adv Ther. 2018 Jan;35(1):43-55. doi: 10.1007/s12325-017-0651-3. Epub 2018 Jan 8.
Usage patterns and effectiveness of a longer-acting formulation of insulin glargine at a strength of 300 units per milliliter (Gla-300) have not been studied in real-world clinical practice. This study evaluated differences in dosing and clinical outcomes before and after Gla-300 treatment initiation in patients with type 2 diabetes starting or switching to treatment with Gla-300 to assess whether the benefits observed in clinical trials translate into real-world settings.
This was a retrospective observational study using medical record data obtained by physician survey for patients starting treatment with insulin glargine at a strength of 100 units per milliliter (Gla-100) or Gla-300, or switching to treatment with Gla-300 from treatment with another basal insulin (BI). Differences in dosing and clinical outcomes before versus after treatment initiation or switching were examined by generalized linear mixed-effects models.
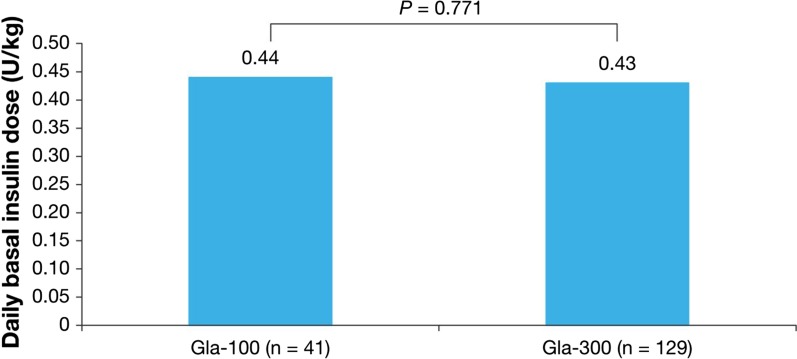
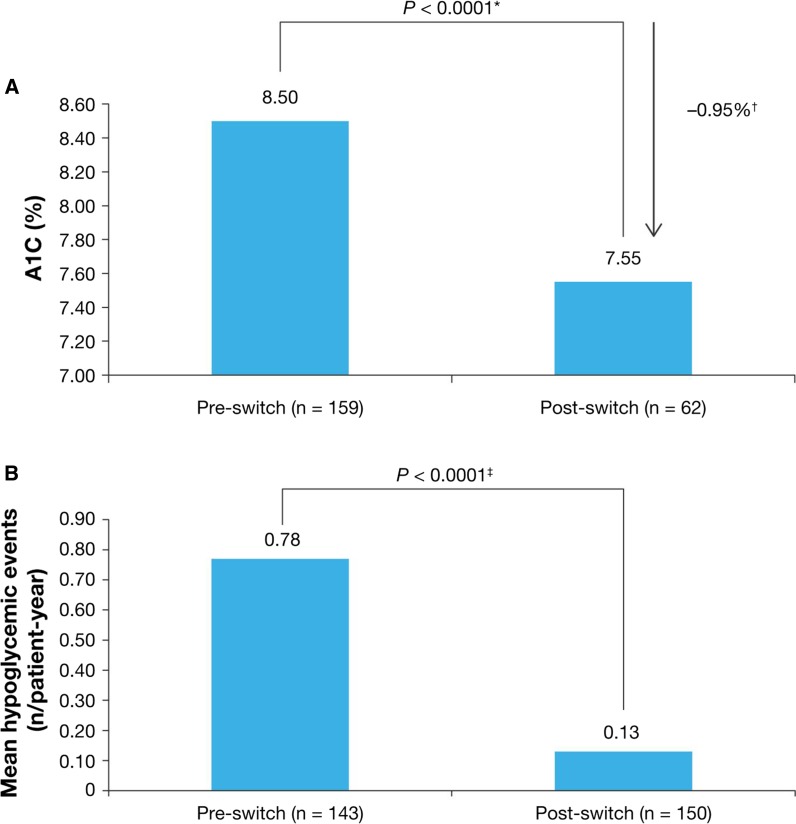
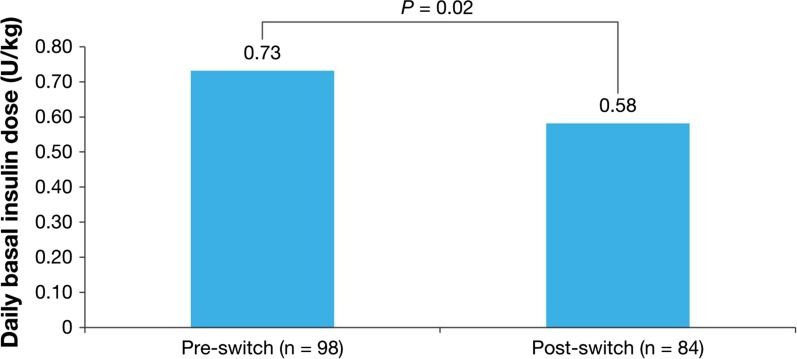
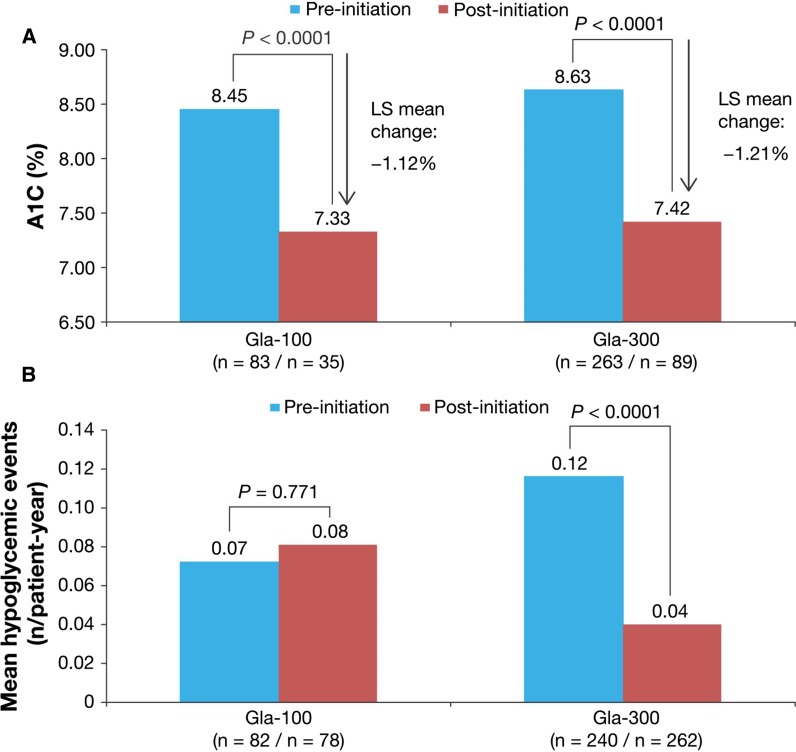
Among insulin-naive patients starting BI treatment, no difference in the final titrated dose was observed in patients starting Gla-300 treatment versus those starting Gla-100 treatment [least-squares (LS) mean 0.43 units per kilogram vs 0.44 units per kilogram; P = 0.77]. Both groups had significant hemoglobin A level reductions (LS mean 1.21 percentage points for Gla-300 and 1.12 percentage points for Gla-100 ; both P < 0.001). The relative risk of hypoglycemic events after Gla-300 treatment initiation was lower than that after Gla-100 treatment initiation [0.31, 95% confidence interval (CI) 0.12-0.81; P = 0.018] at similar daily doses. The daily dose of BI was significantly lower after switching to treatment with Gla-300 from treatment with another BI (0.73 units per kilogram before switch vs 0.58 units per kilogram after switch; P = 0.02). The mean hemoglobin A level was significantly lower after switching than before switching (adjusted difference - 0.95 percentage points, 95% CI - 1.13 to - 0.78 percentage points ; P < 0.0001). Hypoglycemic events per patient-year were significantly lower (relative risk 0.17, 95% CI 0.11-0.26; P < 0.0001).
Insulin-naive patients starting Gla-300 treatment had fewer hypoglycemic events, a similar hemoglobin A level reduction, and no difference in insulin dose versus patients starting Gla-100 treatment. Patients switching to Gla-300 treatment from treatment with other BIs had significantly lower daily doses of BI, with fewer hypoglycemic events, without compromise of hemoglobin A level reduction. These findings suggest Gla-300 in a real-world setting provides benefits in terms of dosing, with improved hemoglobin A level and hypoglycemia rates.
Sanofi US Inc. (Bridgewater, NJ, USA).
在真实的临床实践中,尚未研究过 300 单位/毫升(Gla-300)浓度的长效胰岛素甘精胰岛素的使用模式和疗效。本研究评估了在开始使用甘精胰岛素 300 单位/毫升(Gla-300)治疗或转换为 Gla-300 治疗的 2 型糖尿病患者中,在开始治疗之前和之后剂量和临床结局的差异,以评估临床试验中观察到的益处是否转化为真实环境。
这是一项回顾性观察性研究,使用了通过医生调查获得的病历数据,用于评估开始使用甘精胰岛素 100 单位/毫升(Gla-100)或 Gla-300 治疗的患者,或从其他基础胰岛素(BI)转换为 Gla-300 治疗的患者。通过广义线性混合效应模型检查治疗开始或转换前后剂量和临床结局的差异。
在开始 BI 治疗的胰岛素初治患者中,开始 Gla-300 治疗的患者与开始 Gla-100 治疗的患者的最终滴定剂量无差异[最小二乘(LS)均值分别为每公斤 0.43 单位和 0.44 单位;P=0.77]。两组的血红蛋白 A 水平均显著降低(Gla-300 的 LS 均值为 1.21 个百分点,Gla-100 的 LS 均值为 1.12 个百分点;均 P<0.001)。与 Gla-100 治疗开始后相比,Gla-300 治疗开始后低血糖事件的相对风险较低[0.31,95%置信区间(CI)0.12-0.81;P=0.018],且在相似的每日剂量下。与另一种 BI 治疗转换为 Gla-300 治疗后,BI 的每日剂量显著降低(转换前为 0.73 单位/公斤,转换后为 0.58 单位/公斤;P=0.02)。与转换前相比,转换后平均血红蛋白 A 水平显著降低(调整差异-0.95 个百分点,95%CI-1.13 至-0.78 个百分点;P<0.0001)。每位患者年的低血糖事件显著减少(相对风险 0.17,95%CI 0.11-0.26;P<0.0001)。
开始 Gla-300 治疗的胰岛素初治患者低血糖事件更少,血红蛋白 A 水平降低相似,且胰岛素剂量与开始 Gla-100 治疗的患者无差异。与其他 BI 治疗转换为 Gla-300 治疗的患者,BI 的每日剂量显著降低,低血糖事件减少,而血红蛋白 A 水平降低不受影响。这些发现表明,在真实环境中,Gla-300 在剂量方面具有优势,同时提高了血红蛋白 A 水平和低血糖发生率。
赛诺菲美国公司(美国新泽西州桥水)。