Paterno Mark V, Huang Bin, Thomas Staci, Hewett Timothy E, Schmitt Laura C
Division of Occupational Therapy and Physical Therapy, Cincinnati Children's Hospital Medical Center, Cincinnati, Ohio, USA.
Division of Sports Medicine, Cincinnati Children's Hospital Medical Center, Cincinnati, Ohio, USA.
Orthop J Sports Med. 2017 Dec 19;5(12):2325967117745279. doi: 10.1177/2325967117745279. eCollection 2017 Dec.
Biomechanical predictors of a second anterior cruciate ligament (ACL) injury after ACL reconstruction (ACLR) and return to sport (RTS) have been identified; however, these measures may not be feasible in a standard clinical environment.
PURPOSE/HYPOTHESIS: The purpose of this study was to evaluate whether standard clinical measures predicted the risk of second ACL injuries. The hypothesis tested was that a combination of strength, function, and patient-reported measures at the time of RTS would predict the risk of second ACL injuries with high sensitivity and specificity.
Case-control study; Level of evidence, 3 and Cohort study (prognosis); Level of evidence, 1.
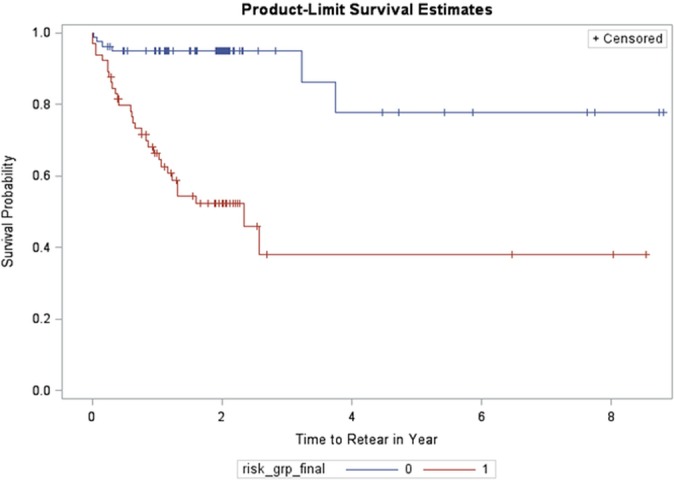
A total of 163 participants (mean age, 16.7 ± 3.0 years) who underwent primary ACLR and were able to RTS were evaluated. All participants completed an assessment of isokinetic strength, hop testing, balance, and the Knee Injury and Osteoarthritis Outcome Score (KOOS). Participants were tracked for a minimum of 24 months to identify occurrences of a second ACL injury. The initial 120 participants enrolled were used to develop a clinical prediction model that utilized classification and regression tree (CART) analysis, and the remaining 43 participants enrolled were used as a validation dataset. Additional analyses were performed in all 163 participants using Kaplan-Meier analysis and Cox proportional hazards modeling.
Approximately 20% (23/114) of the initial subset of the cohort suffered a second ACL injury. CART analysis identified age, sex, knee-related confidence, and performance on the triple hop for distance at the time of RTS as the primary predictors of a second ACL injury. Using these variables, a model was generated from which high-risk (n = 53) and low-risk groups (n = 61) were identified. A total of 22 participants in the high-risk group and 1 participant in the low-risk group suffered a second ACL injury. High-risk participants fit 1 of 2 profiles: (1) age <19 years, triple hop for distance between 1.34 and 1.90 times body height, and triple hop for distance limb symmetry index (LSI) <98.5% (n = 43) or (2) age <19 years, triple hop for distance >1.34 times body height, triple hop for distance LSI >98.5%, female sex, and high knee-related confidence (n = 10). The validation step identified the high-risk group as being 5 times (odds ratio, 5.14 [95% CI, 1.00-26.46]) more likely to suffer a second ACL injury, with a sensitivity of 66.7% and specificity of 72.0%.
These findings recognize measures that accurately identify young patients at high risk of sustaining a second ACL injury within 24 months after RTS. The development of a clinical decision algorithm to identify high-risk patients, inclusive of clinically feasible variables such as age, sex, confidence, and performance on the triple hop for distance, can serve as a foundation to re-evaluate appropriate discharge criteria for RTS.
前交叉韧带重建术(ACLR)后二次前交叉韧带(ACL)损伤及恢复运动(RTS)的生物力学预测指标已被确定;然而,在标准临床环境中,这些指标可能并不适用。
目的/假设:本研究旨在评估标准临床指标是否能预测二次ACL损伤的风险。所检验的假设为,RTS时力量、功能及患者报告指标的综合可高灵敏度和特异性地预测二次ACL损伤的风险。
病例对照研究;证据等级3和队列研究(预后);证据等级1。
共评估了163例接受初次ACLR且能够RTS的参与者(平均年龄16.7±3.0岁)。所有参与者均完成了等速肌力、单腿跳测试、平衡及膝关节损伤和骨关节炎疗效评分(KOOS)评估。对参与者进行至少24个月的随访,以确定二次ACL损伤的发生情况。最初纳入的120例参与者用于建立一个利用分类与回归树(CART)分析的临床预测模型,其余纳入的43例参与者用作验证数据集。对全部163例参与者进行了Kaplan-Meier分析和Cox比例风险建模的额外分析。
该队列初始亚组中约20%(23/114)发生了二次ACL损伤。CART分析确定年龄、性别、膝关节相关信心及RTS时的三级跳远成绩为二次ACL损伤的主要预测指标。利用这些变量生成了一个模型,从中确定了高风险组(n = 53)和低风险组(n = 61)。高风险组中有22例参与者和低风险组中有1例参与者发生了二次ACL损伤。高风险参与者符合以下两种情况之一:(1)年龄<19岁,三级跳远成绩为身高的1.34至1.90倍,且三级跳远肢体对称指数(LSI)<98.5%(n = 43)或(2)年龄<19岁,三级跳远成绩>身高的1.34倍,三级跳远LSI>98.5%,女性,且膝关节相关信心高(n = 10)。验证步骤确定高风险组发生二次ACL损伤的可能性高5倍(比值比,5.14 [95% CI,1.00 - 26.46]),灵敏度为66.7%,特异性为72.0%。
这些发现确定了能准确识别RTS后24个月内有二次ACL损伤高风险年轻患者的指标。开发一种临床决策算法以识别高风险患者,纳入年龄、性别、信心及三级跳远成绩等临床可行变量,可为重新评估RTS的合适出院标准奠定基础。