Division of Hematologic Malignancies, Dana-Farber Cancer Institute and Harvard Medical School, Boston, MA
Department of Biostatistics and Computational Biology, Dana-Farber Cancer Institute and Harvard School of Public Health, Boston, MA.
Haematologica. 2018 Mar;103(3):522-530. doi: 10.3324/haematol.2017.176859. Epub 2018 Jan 11.
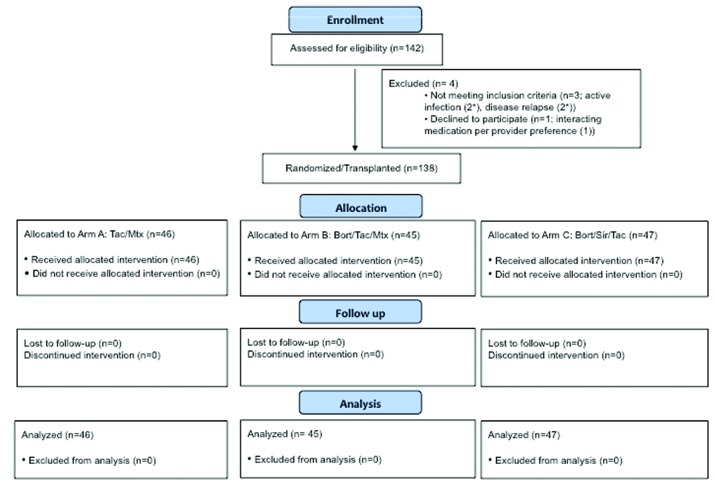
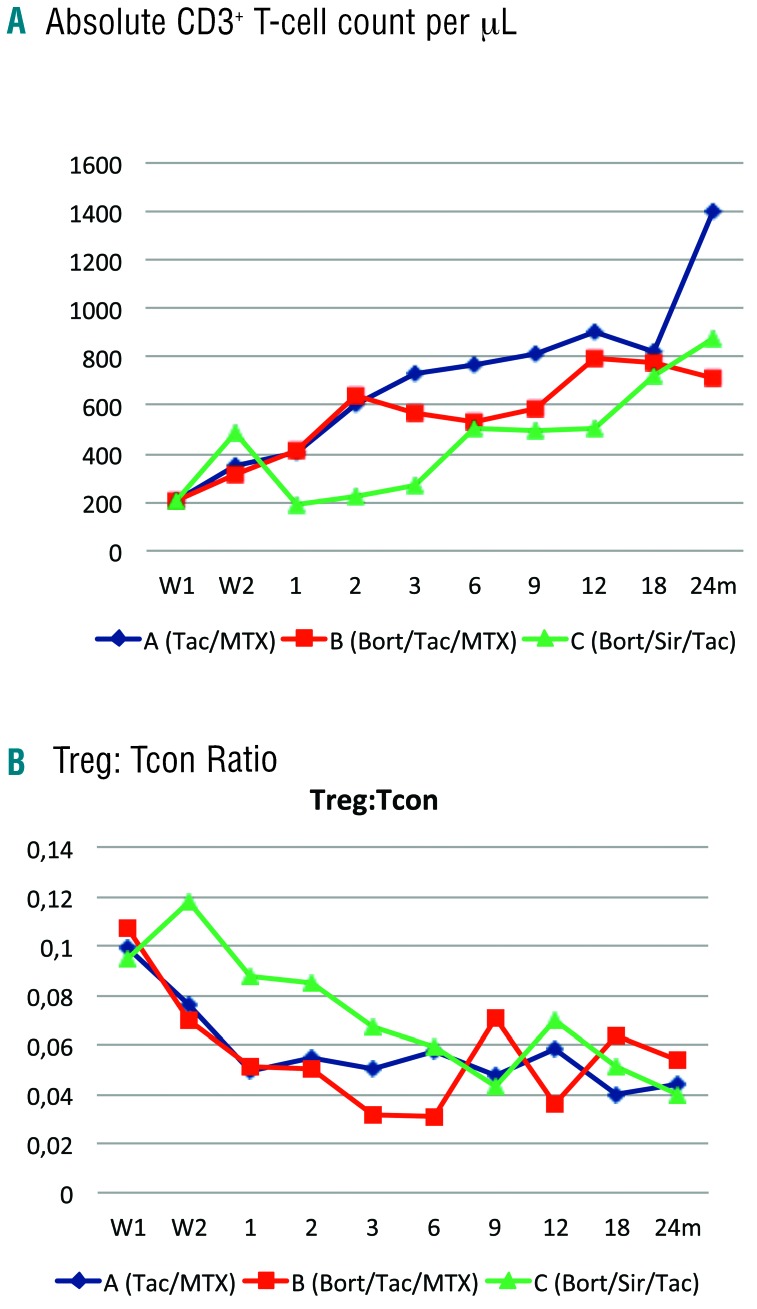
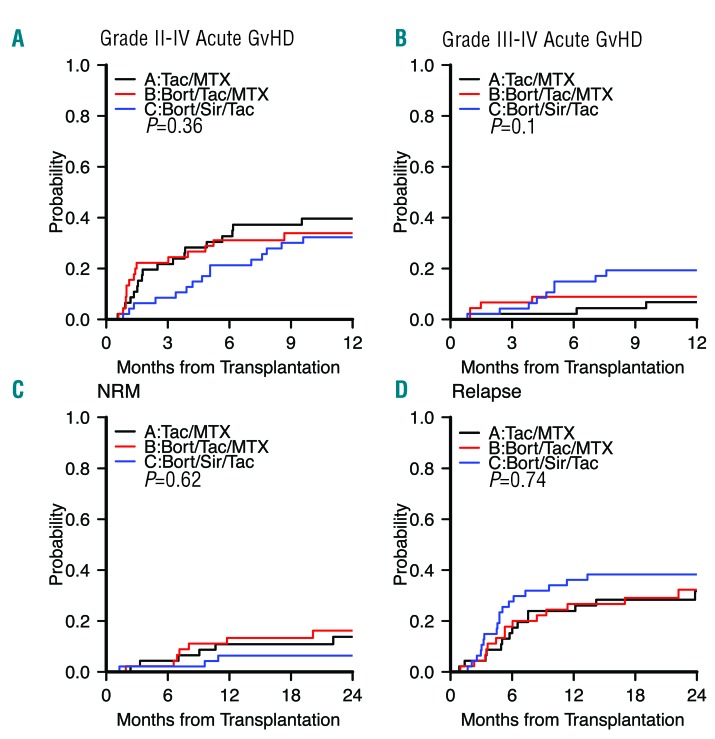
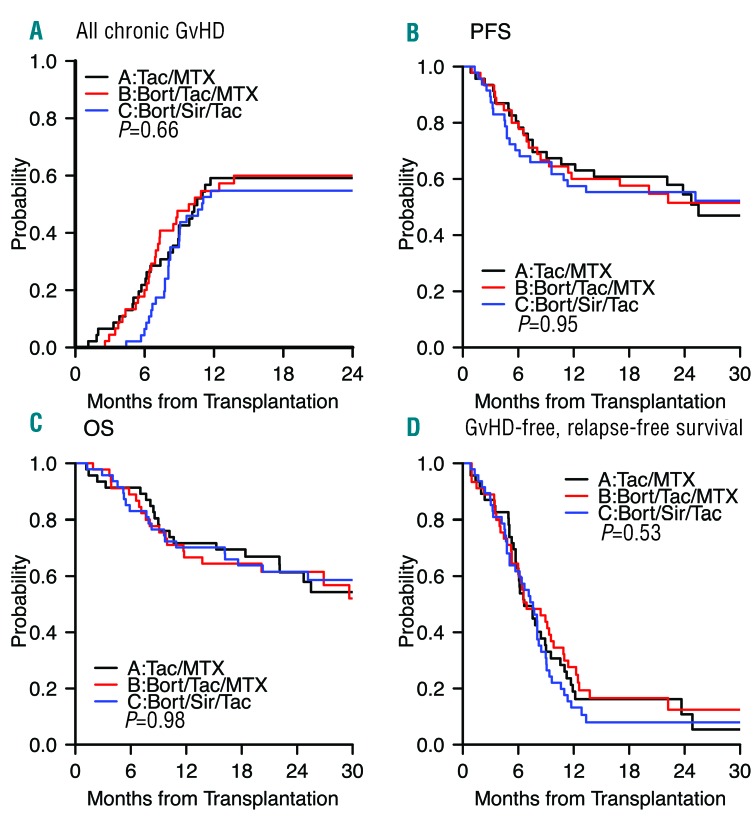
Aprior phase I/II trial of bortezomib/tacrolimus/methotrexate prophylaxis after human leukocyte antigen (HLA)-mismatched reduced intensity conditioning allogeneic hematopoietic stem cell transplantation documented low acute graft--host disease incidence, with promising overall and progression-free survival. We performed an open-label three-arm 1:1:1 phase II randomized controlled trial comparing grade II-IV acute graft--host disease between conventional tacrolimus/methotrexate (A) bortezomib/tacrolimus/methotrexate (B), and bortezomib/sirolimus/tacrolimus (C), in reduced intensity conditioning allogeneic transplantation recipients lacking HLA-matched related donors. The primary endpoint was grade II-IV acute graft--host disease incidence rate by day +180. One hundred and thirty-eight patients (A 46, B 45, C 47) with a median age of 64 years (range: 24-75), varying malignant diagnoses and disease risk (low 14, intermediate 96, high/very high 28) received 7-8/8 HLA-mismatched (40) or matched unrelated donor (98) grafts. Median follow up in survivors was 30 months (range: 14-46). Despite early immune reconstitution differences, day +180 grade II-IV acute graft--host disease rates were similar (A 32.6%, B 31.1%, C 21%; =0.53 for A B, =0.16 for A C). The 2-year non-relapse mortality incidence was similar (A 14%, B 16%, C 6.4%; =0.62), as were relapse (A 32%, B 32%, C 38%; =0.74), chronic graft--host disease (A 59%, B 60% C 55%; =0.66), progression-free survival (A 54%, B 52%, C 55%; =0.95), and overall survival (A 61%, B 62%, C 62%; =0.98). Overall, the bortezomib-based regimens evaluated did not improve outcomes compared with tacrolimus/methotrexate therapy. .
前期 I/II 期试验表明,在 HLA 错配的减低强度预处理异基因造血干细胞移植后,硼替佐米/他克莫司/甲氨蝶呤预防方案可降低急性移植物抗宿主病(GVHD)的发生率,且具有较好的总生存率和无进展生存率。我们进行了一项开放标签的三臂 1:1:1 期 II 随机对照试验,比较了在缺乏 HLA 匹配相关供体的减低强度预处理异基因移植受者中,常规他克莫司/甲氨蝶呤(A)、硼替佐米/他克莫司/甲氨蝶呤(B)和硼替佐米/西罗莫司/他克莫司(C)三种方案的 II-IV 级急性 GVHD 发生率。主要终点是第 180 天的 II-IV 级急性 GVHD 发生率。138 例患者(A 组 46 例,B 组 45 例,C 组 47 例)的中位年龄为 64 岁(范围:24-75 岁),具有不同的恶性诊断和疾病风险(低危 14 例,中危 96 例,高危/极高危 28 例),接受了 7-8/8 HLA 错配(40 例)或匹配的无关供体(98 例)移植。幸存者的中位随访时间为 30 个月(范围:14-46 个月)。尽管早期免疫重建存在差异,但第 180 天 II-IV 级急性 GVHD 发生率相似(A 组 32.6%,B 组 31.1%,C 组 21%;A 与 B 组比较,=0.53;A 与 C 组比较,=0.16)。2 年非复发死亡率相似(A 组 14%,B 组 16%,C 组 6.4%;A 与 B 组比较,=0.62;A 与 C 组比较,=0.16),复发率相似(A 组 32%,B 组 32%,C 组 38%;A 与 B 组比较,=0.74;A 与 C 组比较,=0.16),慢性 GVHD 相似(A 组 59%,B 组 60%,C 组 55%;A 与 B 组比较,=0.66;A 与 C 组比较,=0.16),无进展生存率相似(A 组 54%,B 组 52%,C 组 55%;A 与 B 组比较,=0.95;A 与 C 组比较,=0.16),总生存率相似(A 组 61%,B 组 62%,C 组 62%;A 与 B 组比较,=0.98;A 与 C 组比较,=0.16)。总的来说,与他克莫司/甲氨蝶呤治疗相比,硼替佐米为基础的方案并未改善结局。