Lawerman Tjitske F, Brandsma Rick, Verbeek Renate J, van der Hoeven Johannes H, Lunsing Roelineke J, Kremer Hubertus P H, Sival Deborah A
Departments of Pediatrics and Neurology, Beatrix Children's Hospital, University Medical Center Groningen, Groningen, Netherlands.
Front Hum Neurosci. 2017 Dec 13;11:605. doi: 10.3389/fnhum.2017.00605. eCollection 2017.
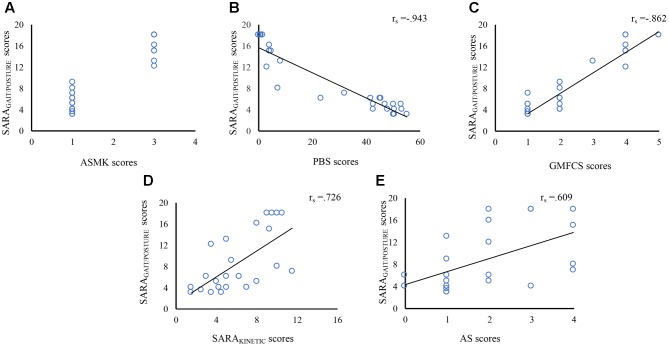
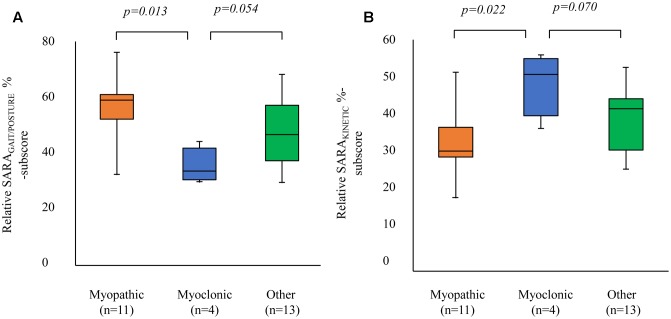
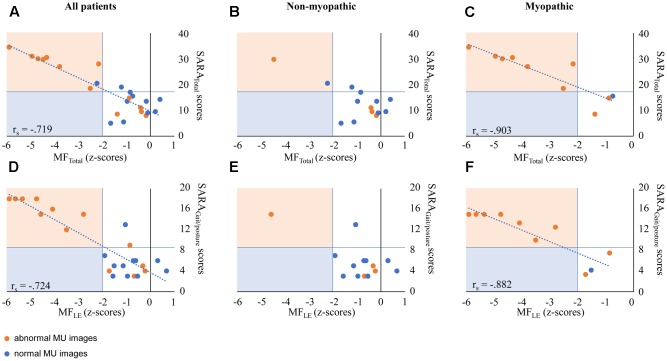
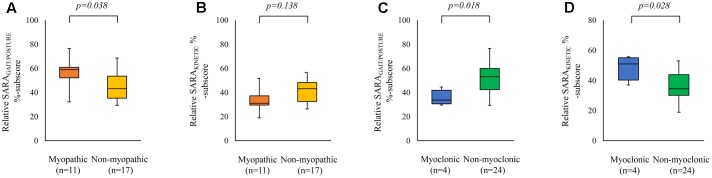
In children, gait and posture assessment provides a crucial marker for the early characterization, surveillance and treatment evaluation of early onset ataxia (EOA). For reliable data entry of studies targeting at gait and posture improvement, uniform quantitative biomarkers are necessary. Until now, the pediatric test construct of gait and posture scores of the Scale for Assessment and Rating of Ataxia sub-scale (SARA) is still unclear. In the present study, we aimed to validate the construct validity and reliability of the pediatric (SARA) sub-scale. We included 28 EOA patients [15.5 (6-34) years; median (range)]. For inter-observer reliability, we determined the ICC on EOA SARA sub-scores by three independent pediatric neurologists. For convergent validity, we associated SARA sub-scores with: (1) Ataxic gait Severity Measurement by Klockgether (ASMK; dynamic balance), (2) Pediatric Balance Scale (PBS; static balance), (3) Gross Motor Function Classification Scale -extended and revised version (GMFCS-E&R), (4) SARA-kinetic scores (SARA; kinetic function of the upper lower limbs), (5) Archimedes Spiral (AS; kinetic function of the upper limbs), and (6) total SARA scores (SARA; i.e., summed SARA, SARA, and SARA sub-scores). For discriminant validity, we investigated whether EOA co-morbidity factors (myopathy and myoclonus) could influence SARA sub-scores. The inter-observer agreement (ICC) on EOA SARA sub-scores was high (0.97). SARA was strongly correlated with the other ataxia and functional scales [ASMK ( = -0.819; < 0.001); PBS ( = -0.943; < 0.001); GMFCS-E&R ( = -0.862; < 0.001); SARA ( = 0.726; < 0.001); AS ( = 0.609; = 0.002); and SARA ( = 0.935; < 0.001)]. Comorbid myopathy influenced SARA scores by concurrent muscle weakness, whereas comorbid myoclonus predominantly influenced SARA scores. In young EOA patients, separate SARA parameters reveal a good inter-observer agreement and convergent validity, implicating the reliability of the scale. In perspective of incomplete discriminant validity, it is advisable to interpret SARA scores for comorbid muscle weakness.
在儿童中,步态和姿势评估为早发性共济失调(EOA)的早期特征描述、监测及治疗评估提供了关键指标。对于旨在改善步态和姿势的研究,可靠的数据录入需要统一的定量生物标志物。到目前为止,共济失调评估与评分量表(SARA)子量表中步态和姿势评分的儿科测试结构仍不明确。在本研究中,我们旨在验证儿科(SARA)子量表的结构效度和信度。我们纳入了28例EOA患者[15.5(6 - 34)岁;中位数(范围)]。对于观察者间信度,我们由三位独立的儿科神经科医生确定EOA SARA子评分的组内相关系数(ICC)。对于收敛效度,我们将SARA子评分与以下各项相关联:(1)Klockgether的共济失调步态严重程度测量(ASMK;动态平衡),(2)儿科平衡量表(PBS;静态平衡),(3)粗大运动功能分类量表 - 扩展和修订版(GMFCS - E&R),(4)SARA - 动力学评分(SARA;上肢和下肢的动力学功能),(5)阿基米德螺旋(AS;上肢的动力学功能),以及(6)SARA总分(SARA;即SARA、SARA和SARA子评分的总和)。对于区分效度,我们研究了EOA合并症因素(肌病和肌阵挛)是否会影响SARA子评分。EOA SARA子评分的观察者间一致性(ICC)很高(0.97)。SARA与其他共济失调和功能量表密切相关[ASMK(r = -0.819;P < 0.001);PBS(r = -0.943;P < 0.001);GMFCS - E&R(r = -0.862;P < 0.