Havsteen Inger, Ovesen Christian, Willer Lasse, Nybing Janus Damm, Ægidius Karen, Marstrand Jacob, Meden Per, Rosenbaum Sverre, Folke Marie Norsker, Christensen Hanne, Christensen Anders
Department of Radiology, Bispebjerg Hospital, Copenhagen University Hospital, Copenhagen, Denmark.
Department of Neurology, Bispebjerg Hospital, Copenhagen University Hospital, Copenhagen, Denmark.
Front Neurol. 2017 Dec 18;8:691. doi: 10.3389/fneur.2017.00691. eCollection 2017.
Diffusion tensor imaging may aid brain ischemia assessment but is more time consuming than conventional diffusion-weighted imaging (DWI). We compared 3-gradient direction DWI (3DWI) and 20-gradient direction DWI (20DWI) standard vendor protocols in a hospital-based prospective cohort of patients with transient ischemic attack (TIA) for lesion detection, lesion brightness, predictability of persisting infarction, and final infarct size.
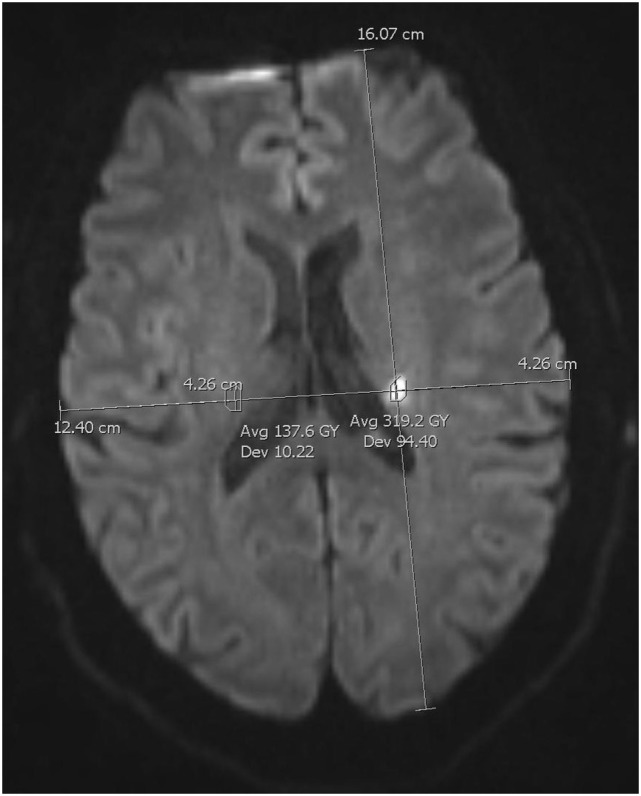
We performed 3T-magnetic resonance imaging including diffusion and T2-fluid attenuated inversion recovery (FLAIR) within 72 h and 8 weeks after ictus. Qualitative lesion brightness was assessed by visual inspection. We measured lesion area and brightness with manual regions of interest and compared with homologous normal tissue.
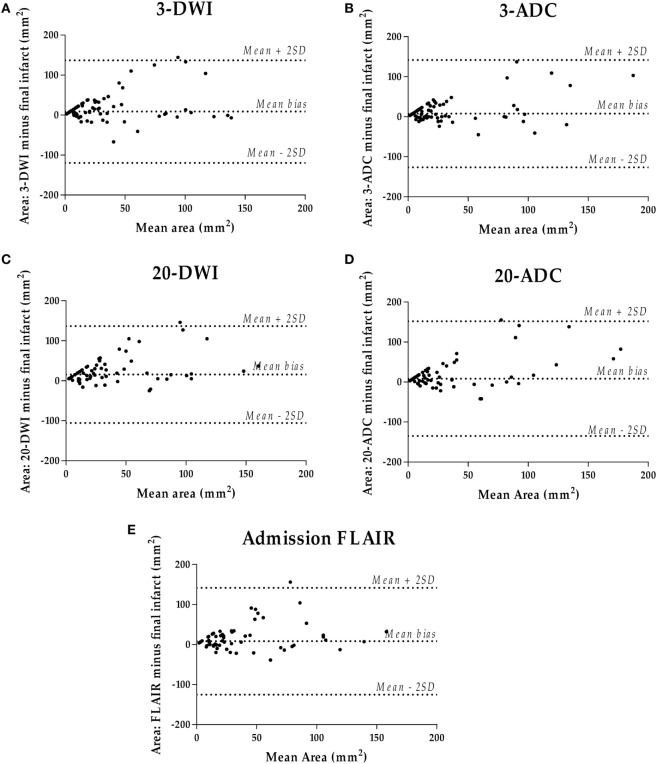
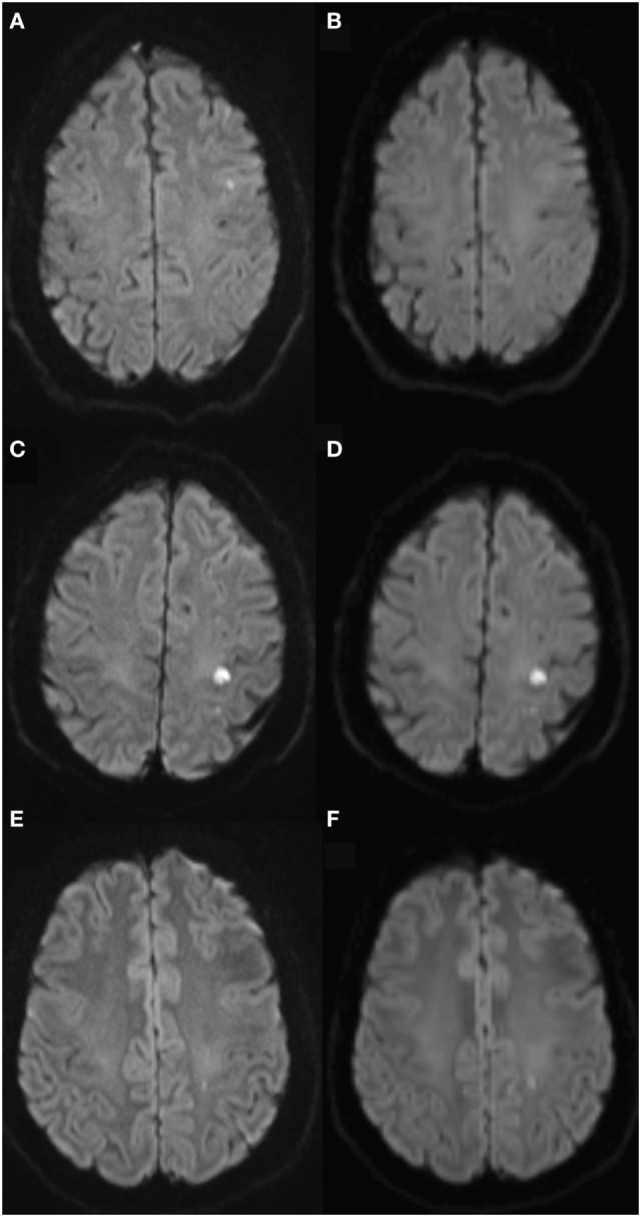
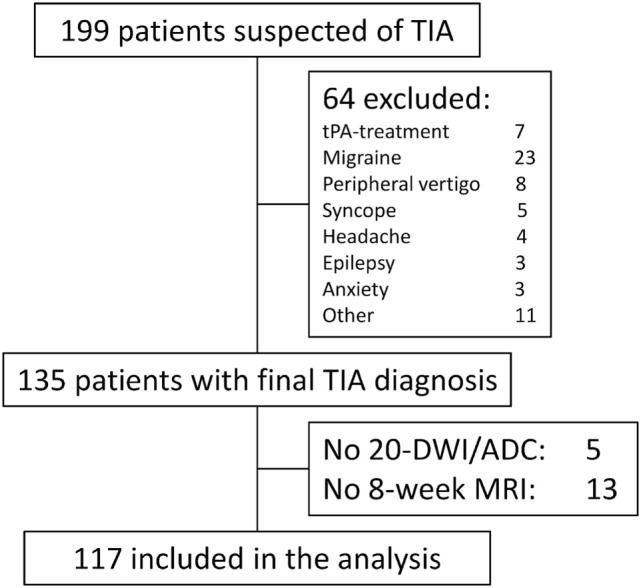
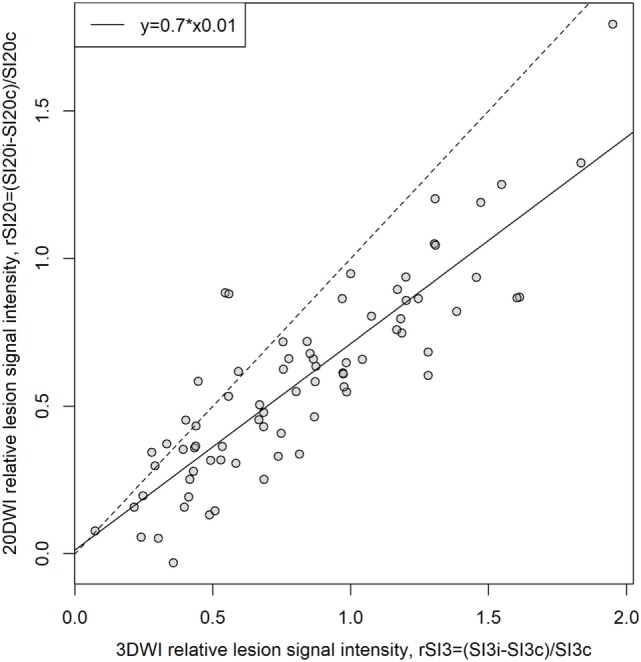
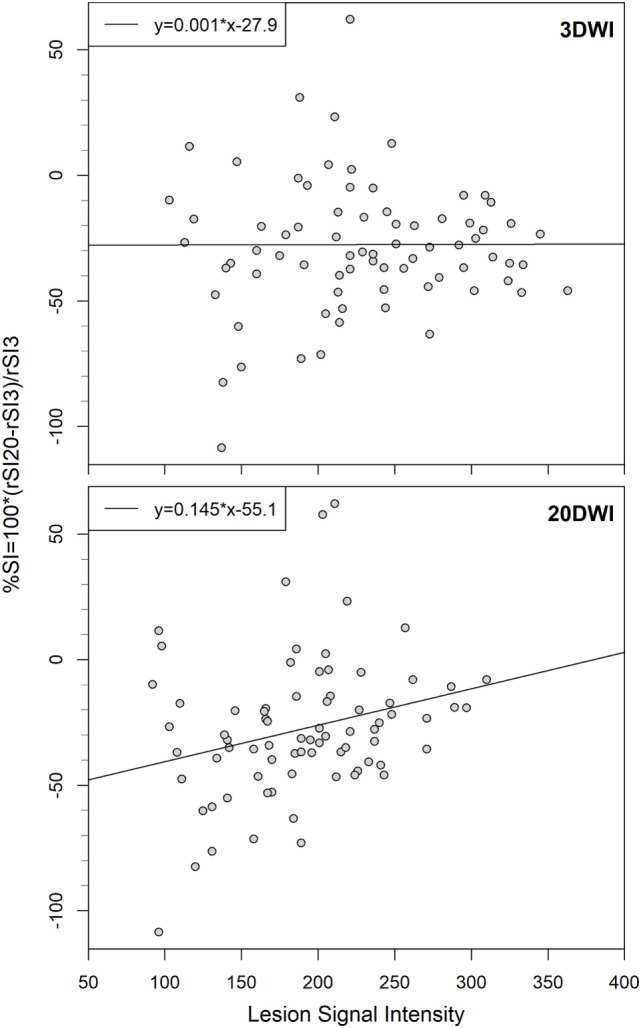
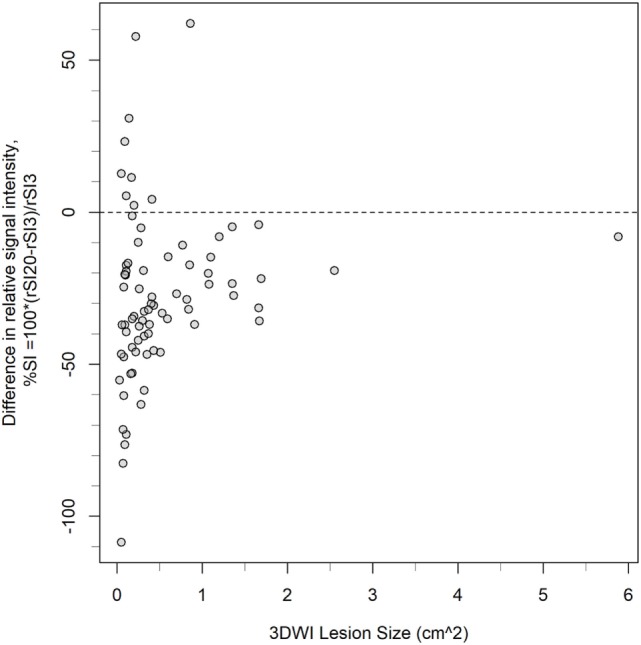
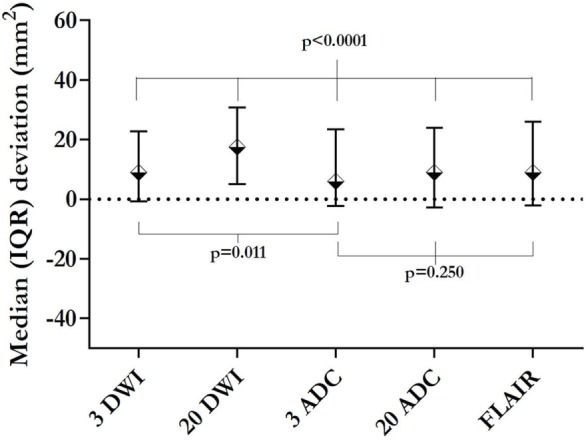
117 patients with clinical TIA showed 78 DWI lesions. 2 lesions showed only on 3DWI. No lesions were uniquely 20DWI positive. 3DWI was visually brightest for 34 lesions. 12 lesions were brightest on 20DWI. The median 3DWI lesion area was larger for lesions equally bright, or brightest on 20DWI [median (IQR) 39 (18-95) versus 18 (10-34) mm, = 0.007]. 3DWI showed highest measured relative lesion signal intensity [median (IQR) 0.77 (0.48-1.17) versus 0.58 (0.34-0.81), = 0.0006]. 3DWI relative lesion signal intensity was not correlated to absolute signal intensity, but 20DWI performed less well for low-contrast lesions. 3DWI lesion size was an independent predictor of persistent infarction. 3-gradient direction apparent diffusion coefficient areas were closest to 8-week FLAIR infarct size.
3DWI detected more lesions and had higher relative lesion SI than 20DWI. 20DWI appeared blurred and did not add information.
http://www.clinicaltrials.gov. Unique Identifier NCT01531946.
扩散张量成像可能有助于脑缺血评估,但比传统扩散加权成像(DWI)耗时更长。我们在一个基于医院的短暂性脑缺血发作(TIA)患者前瞻性队列中,比较了3梯度方向DWI(3DWI)和20梯度方向DWI(20DWI)的标准供应商协议,以检测病变、病变亮度、持续性梗死的可预测性以及最终梗死灶大小。
我们在发病后72小时内和8周时进行了3T磁共振成像,包括扩散成像和T2液体衰减反转恢复(FLAIR)成像。通过视觉检查评估定性病变亮度。我们用手动感兴趣区域测量病变面积和亮度,并与同源正常组织进行比较。
117例临床诊断为TIA的患者显示78个DWI病变。2个病变仅在3DWI上显示。没有病变仅为20DWI阳性。34个病变在3DWI上视觉上最亮。12个病变在20DWI上最亮。对于亮度相同或在20DWI上最亮的病变,3DWI病变面积中位数更大[中位数(四分位间距)39(18 - 95)对18(10 - 34)mm,P = 0.007]。3DWI显示测量的相对病变信号强度最高[中位数(四分位间距)0.77(0.48 - 1.17)对0.58(0.34 - 0.81),P = 0.0006]。3DWI相对病变信号强度与绝对信号强度不相关,但20DWI对低对比度病变的表现较差。3DWI病变大小是持续性梗死的独立预测因素。3梯度方向表观扩散系数区域最接近8周时FLAIR梗死灶大小。
3DWI比20DWI检测到更多病变且相对病变SI更高。20DWI图像显得模糊,并未增加有用信息。