Neale Joshua P H, Pearson James T, Katare Rajesh, Schwenke Daryl O
Department of Physiology-HeartOtago, University of Otago, Dunedin, New Zealand.
Department of Cardiac Physiology, National Cerebral and Cardiovascular Center Research Institute, Suita, Japan.
Front Endocrinol (Lausanne). 2017 Dec 13;8:350. doi: 10.3389/fendo.2017.00350. eCollection 2017.
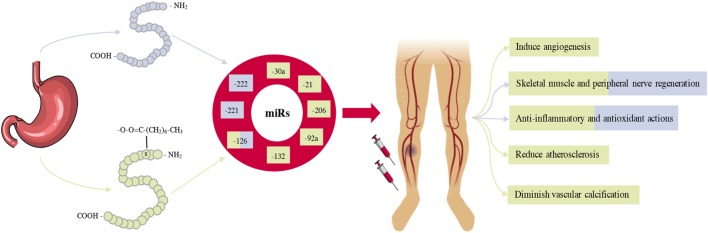
Critical limb ischemia (CLI) is the most severe manifestation of peripheral artery disease. It is characterized by chronic pain at rest, skin ulcerations, and gangrene tissue loss. CLI is a highly morbid condition, resulting in a severely diminished quality of life and a significant risk of mortality. The primary goal of therapy for CLI is to restore blood flow to the affected limb, which is only possible by surgery, but is inadvisable in up to 50% of patients. This subset of patients who are not candidates for revascularisation are referred to as "no-option" patients and are the focus of investigation for novel therapeutic strategies. Angiogenesis, arteriogenesis and vasculogenesis are the processes whereby new blood vessel networks form from the pre-existing vasculature and primordial cells, respectively. In therapeutic angiogenesis, exogenous stimulants are administered to promote angiogenesis and augment limb perfusion, offering a potential treatment option for "no option" patients. However, to date, very few clinical trials of therapeutic angiogenesis in patients with CLI have reported clinically significant results, and it remains a major challenge. Ghrelin, a 28-amino acid peptide, is emerging as a potential novel therapeutic for CLI. In pre-clinical models, exogenous ghrelin has been shown to induce therapeutic angiogenesis, promote muscle regeneration, and reduce oxidative stress the modulation of microRNAs (miRs). miRs are endogenous, small, non-coding ribonucleic acids of ~20-22 nucleotides which regulate gene expression at the post-transcriptional level by either translational inhibition or by messenger ribonucleic acid cleavage. This review focuses on the mounting evidence for the use of ghrelin as a novel therapeutic for CLI, and highlights the miRs which orchestrate these physiological events.
严重肢体缺血(CLI)是外周动脉疾病最严重的表现形式。其特征为静息时的慢性疼痛、皮肤溃疡和坏疽组织缺失。CLI是一种高发病症,会导致生活质量严重下降以及显著的死亡风险。CLI治疗的主要目标是恢复受影响肢体的血流,这只有通过手术才能实现,但高达50%的患者不适合手术。这部分不适合进行血管重建的患者被称为“无选择”患者,是新型治疗策略研究的重点。血管生成、动脉生成和血管发生分别是新血管网络从预先存在的脉管系统和原始细胞形成的过程。在治疗性血管生成中,给予外源性刺激物以促进血管生成并增加肢体灌注,为“无选择”患者提供了一种潜在的治疗选择。然而,迄今为止,很少有关于CLI患者治疗性血管生成的临床试验报告具有临床显著效果,这仍然是一个重大挑战。胃饥饿素是一种由28个氨基酸组成的肽,正逐渐成为CLI的一种潜在新型治疗方法。在临床前模型中,外源性胃饥饿素已被证明可诱导治疗性血管生成、促进肌肉再生并减少氧化应激——对微小RNA(miRs)的调节。miRs是内源性的、小的、约20 - 22个核苷酸的非编码核糖核酸,它们通过翻译抑制或信使核糖核酸切割在转录后水平调节基因表达。本综述重点关注越来越多支持将胃饥饿素用作CLI新型治疗方法的证据,并强调协调这些生理事件的miRs。