Shahrudin Nurul Ain, Mohd Zahidin Aida Zairani, Md Noh Umi Kalthum, Wan Abdul Halim Wan Haslina, Md Din Norshamsiah
Pusat Perubatan Universiti Kebangsaan Malaysia, Cheras, Kuala Lumpur, Malaysia.
GMS Ophthalmol Cases. 2017 Dec 22;7:Doc31. doi: 10.3205/oc000082. eCollection 2017.
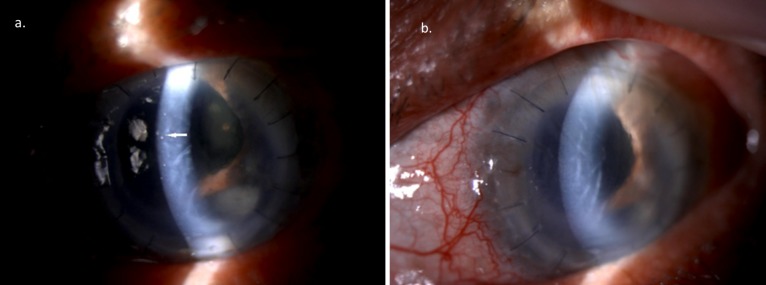
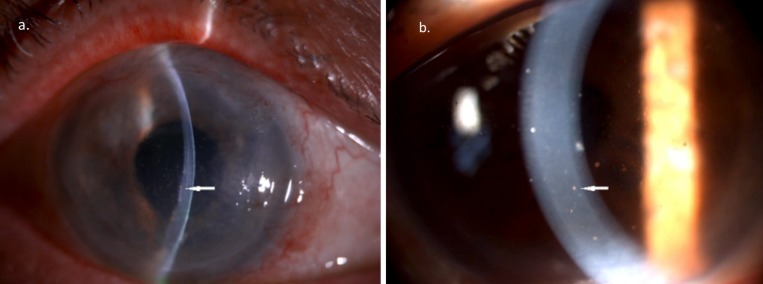
To highlight the clinical presentation of CMV endotheliitis and the challenge in diagnosing this condition in recurrent failed penetrating keratoplasty (PK). Case series There are 3 cases of recurrent failure in PK secondary to CMV endotheliitis presented. Case 1 and 2 were pseudophakic patients, while in case 3, the patient had a previous history of recurrent anterior uveitis. Case 1 and 3 had four and one previous failed PK respectively, while case 2 had endothelial keratoplasty twice before the diagnosis of CMV endotheliitis was made, following positive culture of aqueous humour. The visual acuity ranged from 1/60 to hand movement. All patients had pigmented KP, and two of them had typical coin-shaped KP. Oral valganciclovir was instituted for all patients consisting of 900 mg bidaily for two weeks, followed by 900 mg once daily for six months. Additionally, topical ganciclovir eyedrop 0.5% was given every four hours with topical dexaminim four times a day. Repeated anterior chamber (AC) tap after six months of treatment was negative for CMV in case 3 while cases 1 and 2 are still on treatment. CMV endotheliitis is an increasingly important cause of failed corneal transplant. We recommend anterior chamber tap in suspicious cases of repeatedly failed corneal transplant, regardless of the presence of coin-shaped KP or not. Minimum treatment with oral valganciclovir is important to eradicate the problem, before proceeding with another corneal transplant. It is important to make an accurate early diagnosis by good clinical judgement in preventing loss of corneal endothelial cells. High index of suspicion for CMV endotheliitis as a cause of graft failure must be made especially when the patient presents with coin-shaped KP. Therefore unnecessary treatment resulting from misdiagnosis in these patients can be prevented. Early recognition and treatment of this condition is important to prevent permanent endothelial cell loss and corneal decompensation.
为突出巨细胞病毒(CMV)内皮炎的临床表现以及在复发性穿透性角膜移植术(PK)失败病例中诊断该病所面临的挑战。病例系列 本文报告了3例因CMV内皮炎导致PK复发性失败的病例。病例1和病例2为人工晶状体植入患者,而病例3患者既往有复发性前葡萄膜炎病史。病例1和病例3分别有4次和1次既往PK失败史,病例2在诊断出CMV内皮炎之前曾接受过两次内皮角膜移植术,房水培养呈阳性。视力范围从1/60到手动。所有患者均有色素性角膜后沉着物(KP),其中2例有典型的钱币状KP。所有患者均开始口服缬更昔洛韦,剂量为每日两次,每次900mg,持续两周,随后每日一次,每次900mg,持续六个月。此外,每四小时给予0.5%更昔洛韦滴眼液局部滴眼,同时每日4次给予地塞米松局部滴眼。治疗6个月后,病例3的前房穿刺CMV检测为阴性,而病例1和病例2仍在接受治疗。CMV内皮炎是角膜移植失败的一个日益重要的原因。我们建议,对于反复角膜移植失败的可疑病例,无论是否存在钱币状KP,均应进行前房穿刺。在进行另一次角膜移植之前,使用口服缬更昔洛韦进行最低限度治疗对于根除问题很重要。通过良好的临床判断进行准确的早期诊断对于防止角膜内皮细胞丢失很重要。对于作为移植失败原因的CMV内皮炎必须保持高度怀疑指数,尤其是当患者出现钱币状KP时。因此,可以防止这些患者因误诊而进行不必要的治疗。早期识别和治疗这种疾病对于防止永久性内皮细胞丢失和角膜失代偿很重要。