Chronic Disease Research Group, Minneapolis Medical Research Foundation, Minneapolis, MN; Division of Nephrology, Hennepin County Medical Center, University of Minnesota, Minneapolis, MN.
Chronic Disease Research Group, Minneapolis Medical Research Foundation, Minneapolis, MN.
Am J Kidney Dis. 2018 Jun;71(6):831-841. doi: 10.1053/j.ajkd.2017.10.025. Epub 2018 Jan 10.
Little is known about differences in the clinical course between patients receiving maintenance dialysis who do and do not withdraw from dialysis therapy.
Case-control analysis.
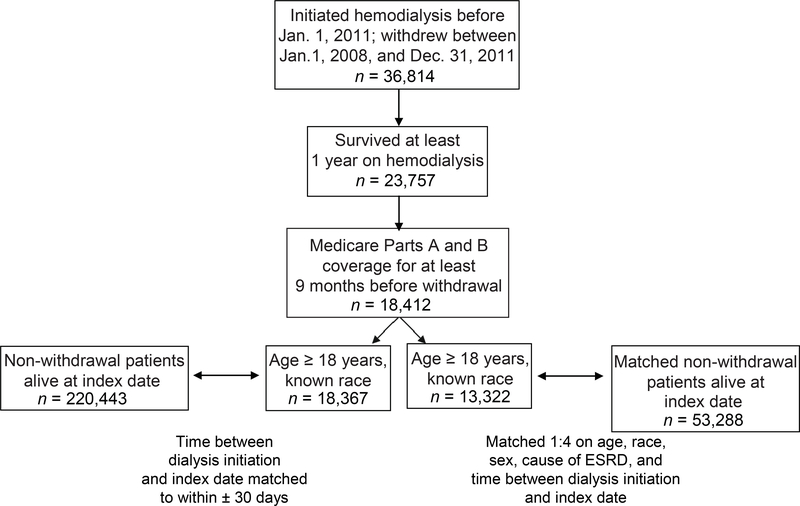
SETTING & PARTICIPANTS: US patients with Medicare coverage who received maintenance hemodialysis for 1 year or longer in 2008 through 2011.
Comorbid conditions, hospitalizations, skilled nursing facility stays, and a morbidity score based on durable medical equipment claims.
Withdrawal from dialysis therapy.
Rates of medical events, hospitalizations, skilled nursing facility stays, and a morbidity score.
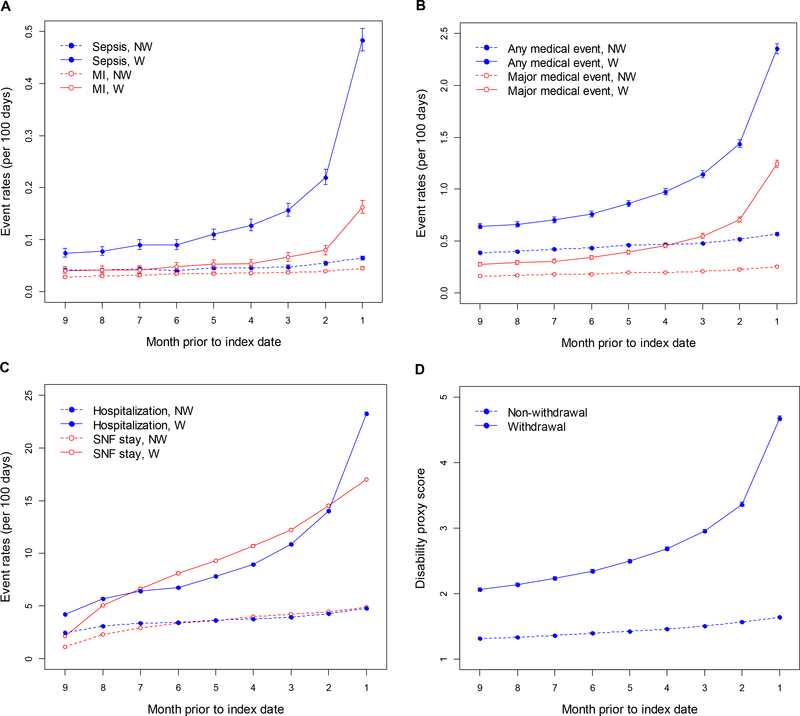
The analysis included 18,367 (7.7%) patients who withdrew and 220,443 (92.3%) who did not. Patients who withdrew were older (mean age, 75.3±11.5 [SD] vs 66.2±14.1 years) and more likely to be women and of white race, and had higher comorbid condition burdens. The odds of withdrawal among women were 7% (95% CI, 4%-11%) higher than among men. Compared to age 65 to 74 years, age 85 years or older was associated with higher adjusted odds of withdrawal (adjusted OR, 1.61; 95% CI, 1.54-1.68), and age 18 to 44 years with lower adjusted odds (adjusted OR, 0.36; 95% CI, 0.32-0.40). Blacks, Asians, and Hispanics were less likely to withdraw than whites (adjusted ORs of 0.36 [95% CI, 0.35-0.38], 0.47 [95% CI, 0.42-0.53], and 0.46 [95% CI, 0.44-0.49], respectively). A higher durable medical equipment claims-based morbidity score was associated with withdrawal, even after adjustment for traditional comorbid conditions and hospitalization; compared to a score of 0 (lowest presumed morbidity), adjusted ORs of withdrawal were 3.48 (95% CI, 3.29-3.67) for a score of 3 to 4 and 12.10 (95% CI, 11.37-12.87) for a score ≥7. Rates of medical events and institutionalization tended to increase in the months preceding withdrawal, as did morbidity score.
Results may not be generalizable beyond US Medicare patients; people who withdrew less than 1 year after dialysis therapy initiation were not studied.
Women, older patients, and those of white race were more likely to withdraw from dialysis therapy. The period before withdrawal was characterized by higher rates of medical events and higher levels of morbidity.
对于接受维持性透析治疗的患者,退出与不退出透析治疗的临床病程差异,目前所知甚少。
病例对照分析。
2008 年至 2011 年期间,在美国接受维持性血液透析治疗 1 年或以上且参加了医疗保险的患者。
合并症、住院、疗养院入住和基于耐用医疗设备索赔的发病率评分。
退出透析治疗。
医疗事件、住院、疗养院入住和发病率评分的发生率。
分析包括 18367 例(7.7%)退出透析治疗的患者和 220443 例(92.3%)未退出的患者。退出透析治疗的患者年龄较大(平均年龄 75.3±11.5[标准差]比 66.2±14.1 岁),更可能为女性和白人,且合并症负担更高。女性退出的几率比男性高 7%(95%置信区间,4%-11%)。与 65 岁至 74 岁相比,85 岁或以上与更高的调整后退出几率相关(调整后的比值比,1.61;95%置信区间,1.54-1.68),而 18 岁至 44 岁与更低的调整后退出几率相关(调整后的比值比,0.36;95%置信区间,0.32-0.40)。黑人、亚洲人和西班牙裔退出的几率低于白人(调整后的比值比分别为 0.36[95%置信区间,0.35-0.38]、0.47[95%置信区间,0.42-0.53]和 0.46[95%置信区间,0.44-0.49])。即使调整了传统合并症和住院情况,基于耐用医疗设备索赔的发病率评分较高也与退出相关;与评分 0(假定发病率最低)相比,评分 3 至 4 的调整后退出比值比为 3.48(95%置信区间,3.29-3.67),评分≥7 的调整后退出比值比为 12.10(95%置信区间,11.37-12.87)。在退出前的几个月,医疗事件和机构化的发生率往往会增加,发病率评分也会增加。
研究结果可能无法推广至美国医疗保险患者以外的人群;未研究退出透析治疗不到 1 年的人群。
女性、老年患者和白人更有可能退出透析治疗。在退出之前,医疗事件的发生率更高,发病率评分也更高。