Department of Epidemiology, Harvard T.H. Chan School of Public Health, Boston, Massachusetts.
Francis I. Proctor Foundation, University of California, San Francisco, California.
AIDS. 2018 Mar 13;32(5):635-643. doi: 10.1097/QAD.0000000000001737.
We investigate the effect of immediate antiretroviral therapy (ART) eligibility on HIV incidence among HIV-uninfected household members.
Regression discontinuity study arising from a population-based cohort.
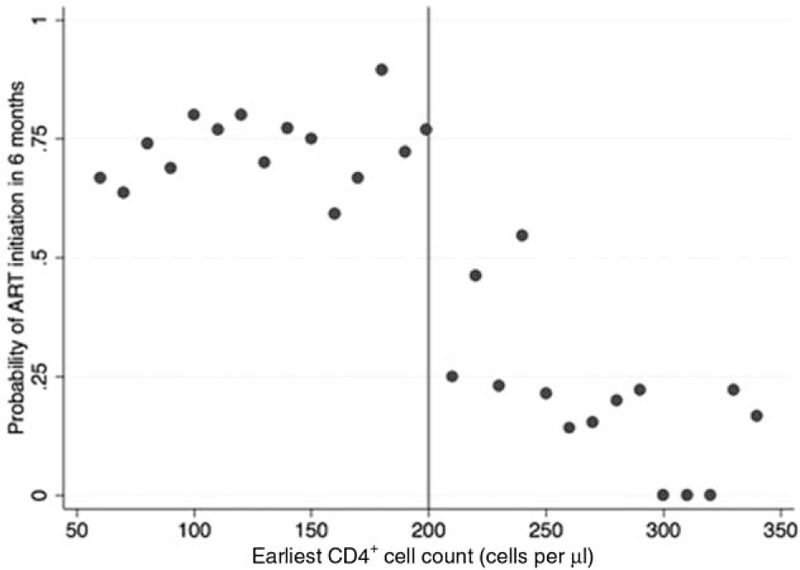
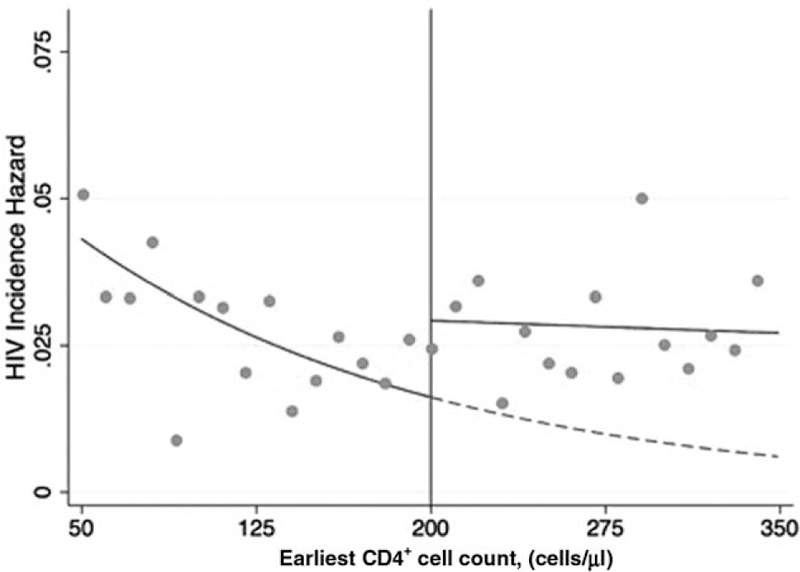
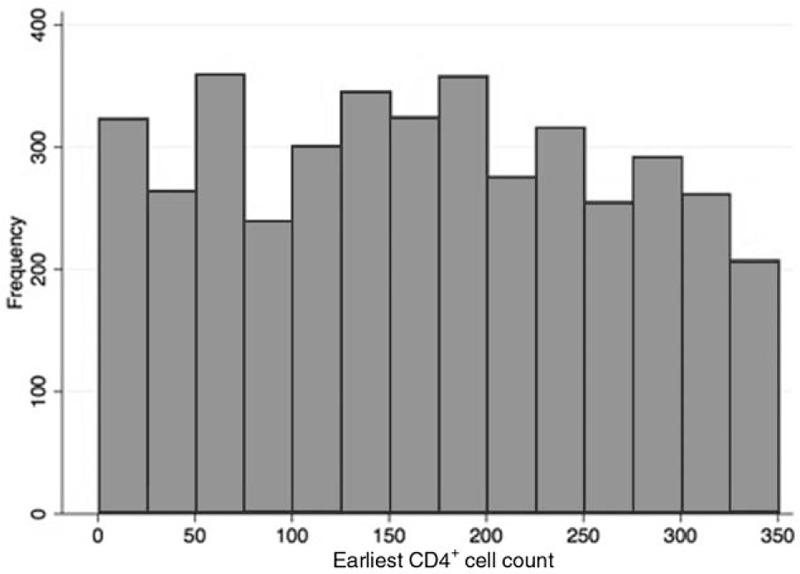
Household members of patients seeking care at the Hlabisa HIV Treatment and Care Programme in rural KwaZulu-Natal South Africa between January 2007 and August 2011 with CD4 cell counts up to 350 cells/μl were eligible for inclusion if they had at least two HIV tests and were HIV-uninfected at the time the index patient linked to care (N = 4115). Regression discontinuity was used to assess the intention-to-treat effect of immediate versus delayed ART eligibility on HIV incidence among household members. Exploiting the CD4 cell count-based threshold rule for ART initiation (CD4 < 200 cells/μl until August 2011), we used Cox proportional hazards models to compare outcomes for household members of patients who presented for care with CD4 cell counts just above versus just below the ART initiation threshold.
Characteristics of household members of index patients initiating HIV care were balanced between those with an index patient immediately eligible for ART (N = 2489) versus delayed for ART (N = 1626). There were 337 incident HIV infections among household members, corresponding to an HIV incidence of 2.4 infections per 100 person-years (95% confidence interval 2.5-3.1). Immediate eligibility for treatment reduced HIV incidence in households by 47% in our optimal estimate (hazard ratio = 0.53, 95% confidence interval 0.30-0.96), and by 32-60% in alternate specifications of the model.
Immediate eligibility of ART led to substantial reductions in household-level HIV incidence.
研究即刻抗逆转录病毒治疗(ART)资格对 HIV 未感染者的 HIV 发病率的影响。
基于人群的队列的回归不连续性研究。
2007 年 1 月至 2011 年 8 月期间,在南非夸祖鲁-纳塔尔省农村 Hlabisa HIV 治疗和护理计划寻求治疗的患者的家庭成员,如果他们至少进行了两次 HIV 检测,并且在索引患者开始接受护理时(N=4115)未感染 HIV,且 CD4 细胞计数高达 350 个/μl,则有资格纳入。使用回归不连续性来评估即刻与延迟 ART 资格对家庭接触者 HIV 发病率的意向治疗效果。利用基于 CD4 细胞计数的 ART 起始阈值规则(直到 2011 年 8 月,CD4<200 个/μl),我们使用 Cox 比例风险模型比较了 CD4 细胞计数略高于与略低于 ART 起始阈值的患者就诊的家庭接触者的结果。
与延迟接受 ART 的患者(N=1626)相比,符合立即接受 ART 资格的患者(N=2489)的索引患者的家庭接触者的特征是平衡的。家庭接触者中有 337 例发生了 HIV 感染,对应的 HIV 发病率为每 100 人年 2.4 例(95%置信区间 2.5-3.1)。在我们的最佳估计中,即刻获得治疗资格使家庭中的 HIV 发病率降低了 47%(风险比=0.53,95%置信区间 0.30-0.96),并且在模型的其他规格中降低了 32-60%。
ART 的即刻资格导致家庭层面的 HIV 发病率大幅降低。