Department of Physical Therapy, University of British Columbia, Vancouver, BC, Canada V6T 1Z3.
Stroke Division, Florey Institute of Neuroscience and Mental Health, University of Melbourne, Melbourne, VIC 3084, Australia.
Neural Plast. 2017;2017:4281532. doi: 10.1155/2017/4281532. Epub 2017 Nov 16.
Severity of arm impairment alone does not explain motor outcomes in people with severe impairment post stroke.
Define the contribution of brain biomarkers to upper limb motor outcomes in people with severe arm impairment post stroke.
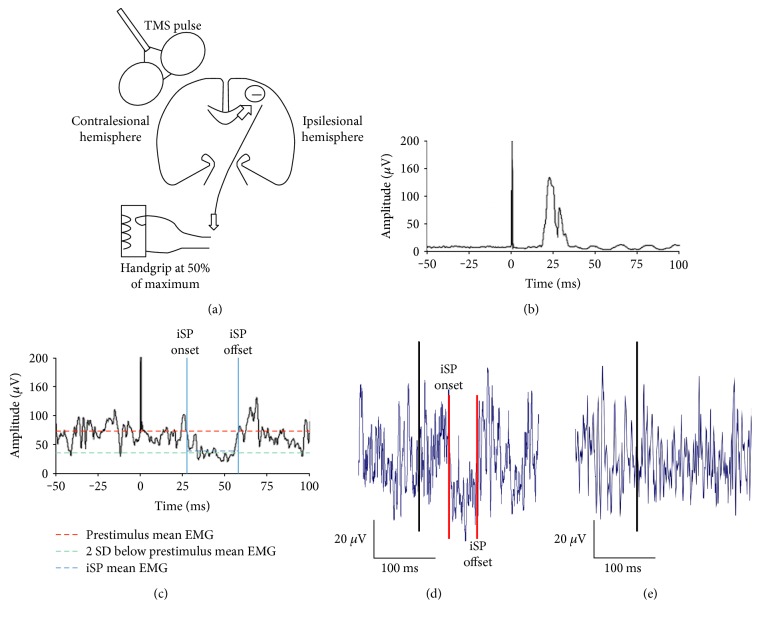
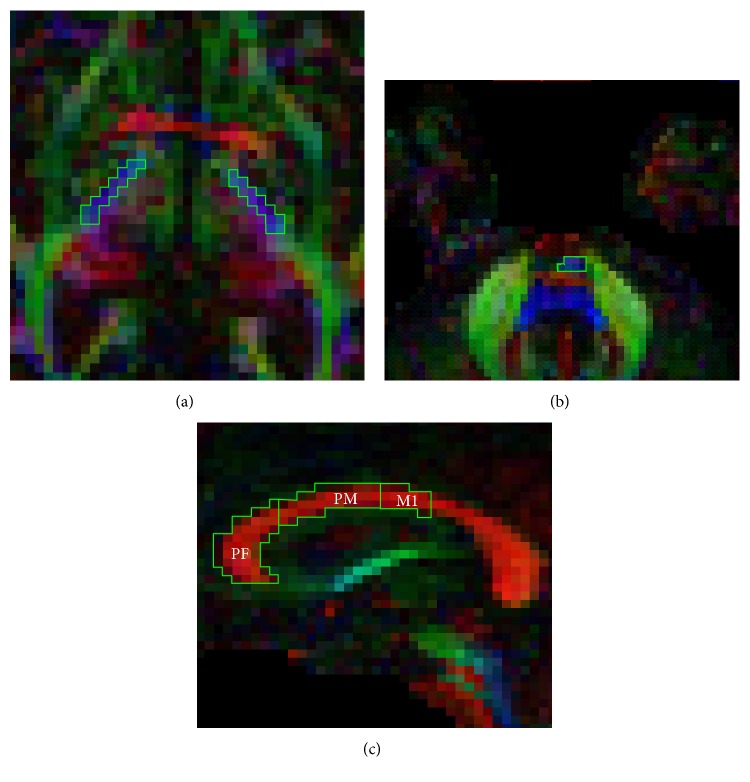
Paretic arm impairment (Fugl-Meyer upper limb, FM-UL) and function (Wolf Motor Function Test rate, WMFT-rate) were measured in 15 individuals with severe (FM-UL ≤ 30/66) and 14 with mild-moderate (FM-UL > 40/66) impairment. Transcranial magnetic stimulation and diffusion weight imaging indexed structure and function of the corticospinal tract and corpus callosum. Separate models of the relationship between possible biomarkers and motor outcomes at a single chronic (≥6 months) time point post stroke were performed.
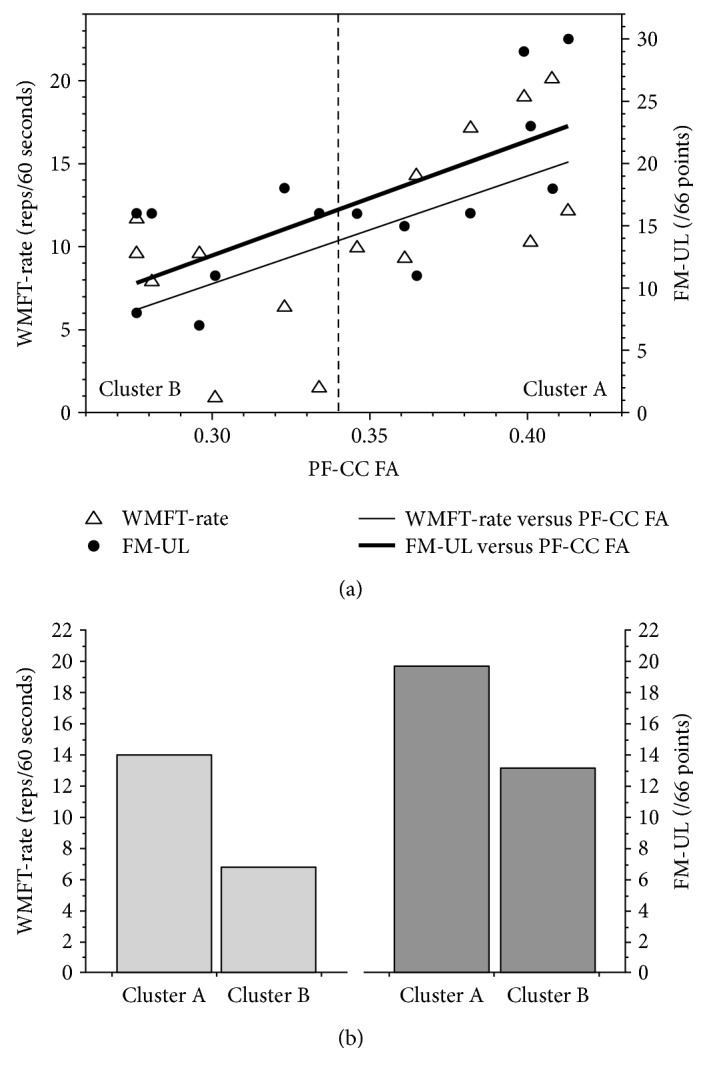
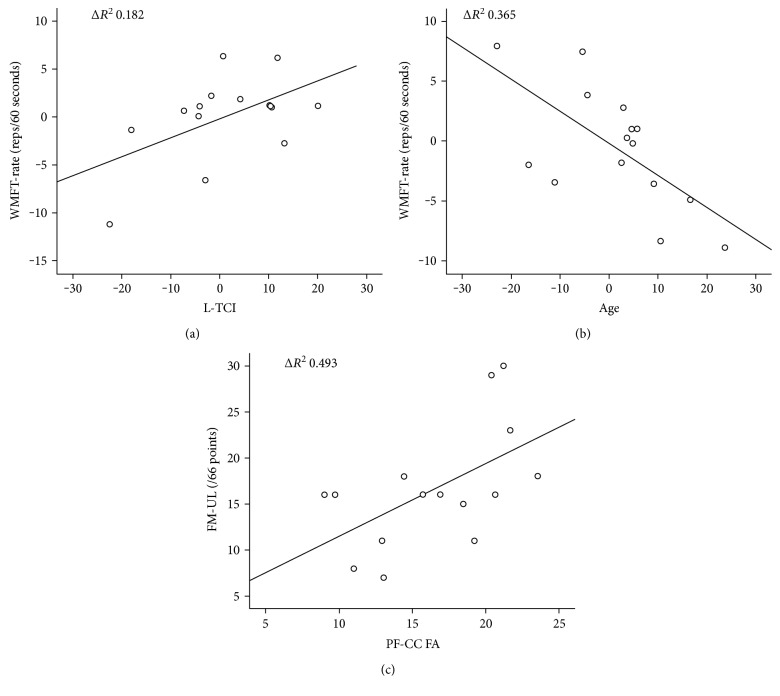
Age (Δ0.365, = 0.017) and ipsilesional-transcallosal inhibition (Δ0.182, = 0.048) explained a 54.7% ( = 0.009) variance in paretic WMFT-rate. Prefrontal corpus callous fractional anisotropy (PF-CC FA) alone explained 49.3% ( = 0.007) variance in FM-UL outcome. The same models did not explain significant variance in mild-moderate stroke. In the severe group, k-means cluster analysis of PF-CC FA distinguished two subgroups, separated by a clinically meaningful and significant difference in motor impairment ( = 0.049) and function ( = 0.006) outcomes.
Corpus callosum function and structure were identified as possible biomarkers of motor outcome in people with chronic and severe arm impairment.
单纯的手臂损伤严重程度并不能解释脑卒中后严重损伤患者的运动预后。
确定脑生物标志物对脑卒中后严重手臂损伤患者上肢运动预后的贡献。
在 15 名严重(FM-UL≤30/66)和 14 名轻度至中度(FM-UL>40/66)损伤的患者中测量了瘫痪手臂的损伤(Fugl-Meyer 上肢,FM-UL)和功能(Wolf 运动功能测试率,WMFT-rate)。经颅磁刺激和弥散张量成像指数皮质脊髓束和胼胝体的结构和功能。在脑卒中后单一慢性(≥6 个月)时间点,对可能的生物标志物与运动结果之间的关系进行了单独的模型分析。
年龄(Δ0.365, = 0.017)和同侧皮质脊髓束抑制(Δ0.182, = 0.048)解释了瘫痪 WMFT-rate 的 54.7%( = 0.009)的变化。额胼胝体分数各向异性(PF-CC FA)单独解释了 FM-UL 结果的 49.3%( = 0.007)的变化。同样的模型不能解释轻度至中度脑卒中的显著变化。在严重组中,PF-CC FA 的 K-均值聚类分析将两个亚组分开,两组在运动损伤( = 0.049)和功能( = 0.006)结果方面存在显著的临床差异。
胼胝体功能和结构被确定为慢性和严重手臂损伤患者运动预后的可能生物标志物。