Verboket R, Leiblein M, Seebach C, Nau C, Janko M, Bellen M, Bönig H, Henrich D, Marzi I
Department of Trauma-, Hand- and Reconstructive Surgery, University Hospital Frankfurt, Frankfurt, Germany.
Department of Transfusion Medicine and Immune Hematology, University Hospital Frankfurt and DRK Blood Donor Service Baden-Württemberg-Hessen, Frankfurt, Germany.
Eur J Trauma Emerg Surg. 2018 Oct;44(5):649-665. doi: 10.1007/s00068-018-0906-y. Epub 2018 Jan 19.
Reconstruction of long segmental bone defects is demanding for patients and surgeons, and associated with long-term treatment periods and substantial complication rates in addition to high costs. While defects up to 4-5 cm length might be filled up with autologous bone graft, heterologous bone from cadavers, or artificial bone graft substitutes, current options to reconstruct bone defects greater than 5 cm consist of either vascularized free bone transfers, the Masquelet technique or the Ilizarov distraction osteogenesis. Alternatively, autologous cell transplantation is an encouraging treatment option for large bone defects as it eliminates problems such as limited autologous bone availability, allogenic bone immunogenicity, and donor-site morbidity, and might be used for stabilizing loose alloplastic implants.
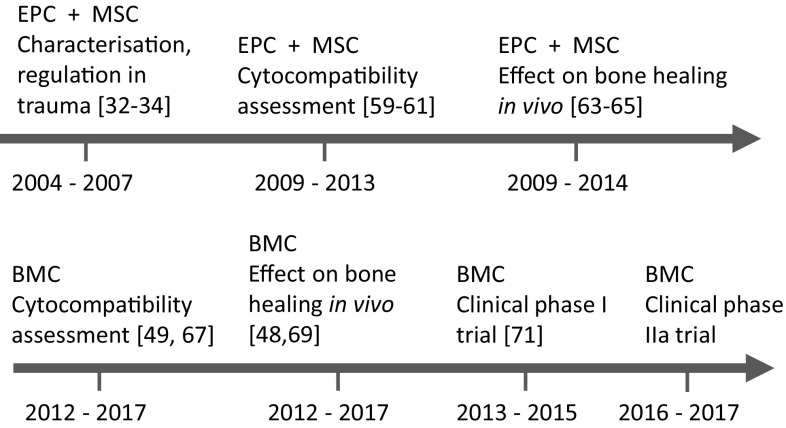
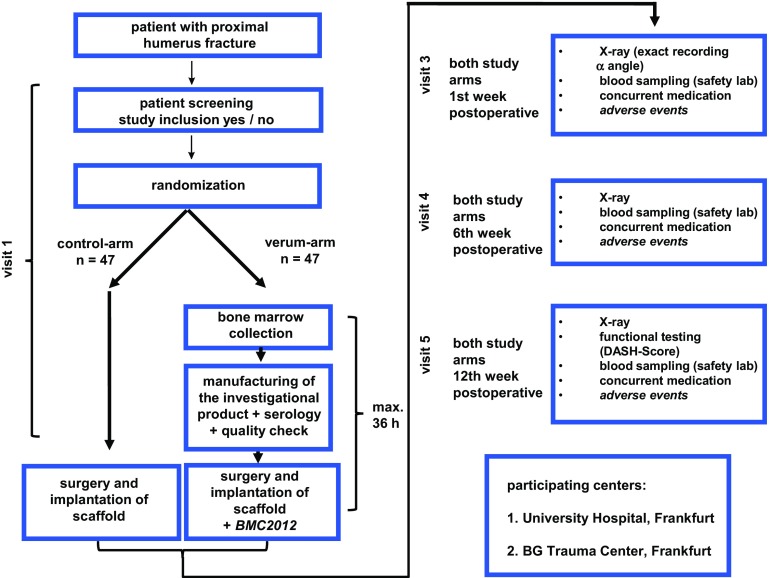
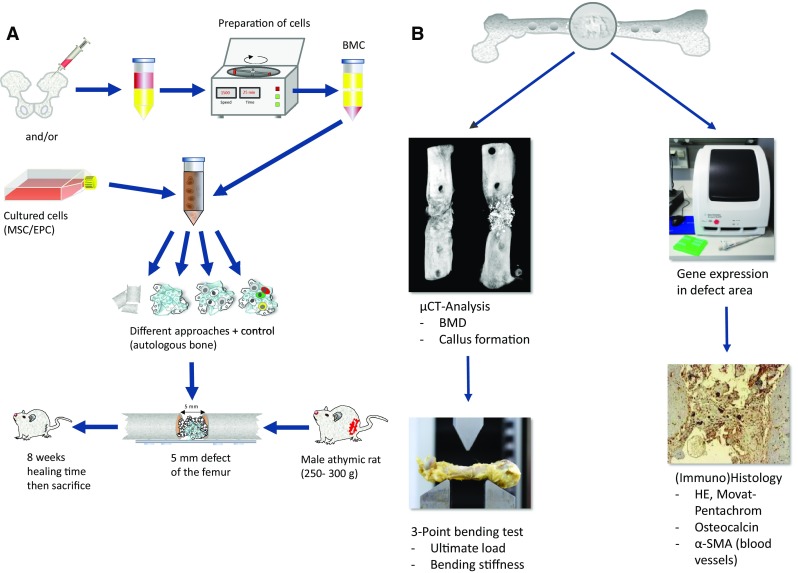
The authors show different cell therapies without expansion in culture, with ex vivo expansion and cell therapy in local bone defects, bone healing and osteonecrosis. Different kinds of cells and scaffolds investigated in our group as well as in vivo transfer studies and BMC used in clinical phase I and IIa clinical trials of our group are shown.
Our research history demonstrated the great potential of various stem cell species to support bone defect healing. It was clearly shown that the combination of different cell types is superior to approaches using single cell types. We further demonstrate that it is feasible to translate preclinically developed protocols from in vitro to in vivo experiments and follow positive convincing results into a clinical setting to use autologous stem cells to support bone healing.
长节段骨缺损的重建对患者和外科医生来说要求很高,不仅治疗周期长、成本高,而且并发症发生率也很高。虽然长度达4 - 5厘米的缺损可以用自体骨移植、尸体的异体骨或人工骨移植替代物填充,但目前重建超过5厘米骨缺损的选择包括带血管蒂的游离骨移植、Masquelet技术或Ilizarov牵张成骨术。另外,自体细胞移植是治疗大骨缺损的一种令人鼓舞的方法,因为它消除了诸如自体骨供应有限、异体骨免疫原性和供区并发症等问题,还可用于稳定松动的异体植入物。
作者展示了不同的细胞治疗方法,包括未经体外扩增的、经体外扩增的以及局部骨缺损、骨愈合和骨坏死的细胞治疗。展示了我们团队研究的不同种类的细胞和支架,以及我们团队在I期和IIa期临床试验中使用的体内移植研究和骨髓细胞。
我们的研究历程证明了各种干细胞在支持骨缺损愈合方面具有巨大潜力。很明显,不同细胞类型的组合优于单一细胞类型的方法。我们进一步证明,将临床前开发的方案从体外实验转化为体内实验,并将令人信服的积极结果应用于临床环境,使用自体干细胞来支持骨愈合是可行的。