Xu Yan, Shoamanesh Ashkan, Schulman Sam, Dowlatshahi Dar, Al-Shahi Salman Rustam, Moldovan Ioana Doina, Wells Philip Stephen, AlKherayf Fahad
Department of Medicine, University of Toronto, Toronto, Canada.
Division of Neurology, Department of Medicine, Population Health Research Institute, McMaster University, Hamilton, Canada.
PLoS One. 2018 Jan 25;13(1):e0191137. doi: 10.1371/journal.pone.0191137. eCollection 2018.
While oral anticoagulants (OACs) are highly effective for ischemic stroke prevention in atrial fibrillation, intracerebral hemorrhage (ICH) remains the most feared complication of OAC. Clinical controversy remains regarding OAC resumption and its timing for ICH survivors with atrial fibrillation because the balance between risks and benefits has not been investigated in randomized trials.
AIMS/HYPOTHESIS: To survey the practice of stroke neurologists, thrombosis experts and neurosurgeons on OAC re-initiation following OAC-associated ICH.
An online survey was distributed to members of the International Society for Thrombosis and Haemostasis, Canadian Stroke Consortium, NAVIGATE-ESUS trial investigators (Clinicatrials.gov identifier NCT02313909) and American Association of Neurological Surgeons. Demographic factors and 11 clinical scenarios were included.
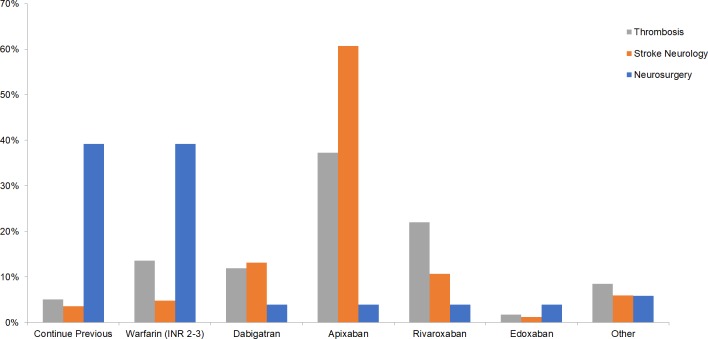
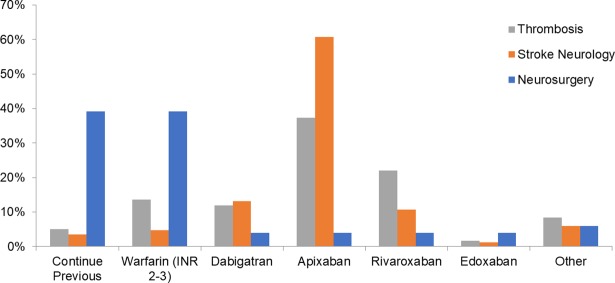
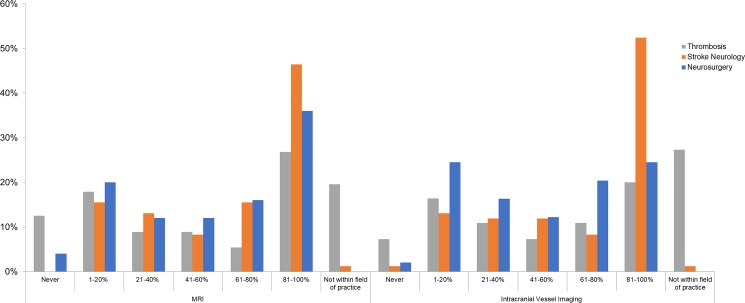
Two hundred twenty-eight participants from 38 countries completed the survey. Majority of participants were affiliated with academic centers, and >20% managed more than 15 OAC-associated ICH patients/year. Proportion of respondents suggesting OAC anticoagulant resumption varied from 30% (for cerebral amyloid angiopathy) to 98% (for traumatic ICH). Within this group, there was wide distribution in response for timing of resumption: 21.4% preferred to re-start OACs after 1-3 weeks of incident ICH, while 25.3% opted to start after 1-3 months. Neurosurgery respondents preferred earlier OAC resumption compared to stroke neurologists or thrombosis experts in 5 scenarios (p<0.05 by Kendall's tau).
Wide variations in current practice exist among management of OAC-associated ICH, with decisions influenced by patient- and provider-related factors. As these variations likely reflect the lack of high quality evidence, randomized trials are direly needed in this population.
虽然口服抗凝药(OACs)在预防心房颤动患者缺血性卒中方面非常有效,但脑出血(ICH)仍然是OAC最令人担忧的并发症。对于心房颤动合并ICH的幸存者,OAC的重新使用及其时机在临床上仍存在争议,因为随机试验尚未对风险和益处之间的平衡进行研究。
目的/假设:调查卒中神经科医生、血栓形成专家和神经外科医生对OAC相关ICH后重新开始使用OAC的做法。
向国际血栓与止血学会、加拿大卒中联盟、NAVIGATE-ESUS试验研究者(Clinicaltrials.gov标识符NCT02313909)和美国神经外科医师协会成员进行在线调查。纳入了人口统计学因素和11种临床情况。
来自38个国家的228名参与者完成了调查。大多数参与者隶属于学术中心,超过20%的参与者每年管理超过15例OAC相关ICH患者。建议重新开始使用OAC抗凝剂的受访者比例从30%(脑淀粉样血管病)到98%(创伤性ICH)不等。在这一组中,重新开始使用的时间选择分布广泛:21.4%的人倾向于在ICH发生后1-3周重新开始使用OAC,而25.3%的人选择在1-3个月后开始使用。在5种情况下,神经外科受访者比卒中神经科医生或血栓形成专家更倾向于更早重新开始使用OAC(肯德尔tau检验,p<0.05)。
OAC相关ICH的管理目前存在很大差异,决策受患者和提供者相关因素影响。由于这些差异可能反映了缺乏高质量证据,因此该人群迫切需要进行随机试验。