Centre for Health Informatics, University of Manchester, Vaughan House, Portsmouth St, Manchester, M13 9GB, UK.
The Manchester Molecular Pathology Innovation Centre, University of Manchester, Manchester, UK.
Alzheimers Res Ther. 2018 Jan 15;10(1):4. doi: 10.1186/s13195-017-0332-0.
Given the complex and progressive nature of Alzheimer's disease (AD), a precision medicine approach for diagnosis and treatment requires the identification of patient subgroups with biomedically distinct and actionable phenotype definitions.
Longitudinal patient-level data for 1160 AD patients receiving placebo or no treatment with a follow-up of up to 18 months were extracted from an integrated clinical trials dataset. We used latent class mixed modelling (LCMM) to identify patient subgroups demonstrating distinct patterns of change over time in disease severity, as measured by the Alzheimer's Disease Assessment Scale-cognitive subscale score. The optimal number of subgroups (classes) was selected by the model which had the lowest Bayesian Information Criterion. Other patient-level variables were used to define these subgroups' distinguishing characteristics and to investigate the interactions between patient characteristics and patterns of disease progression.
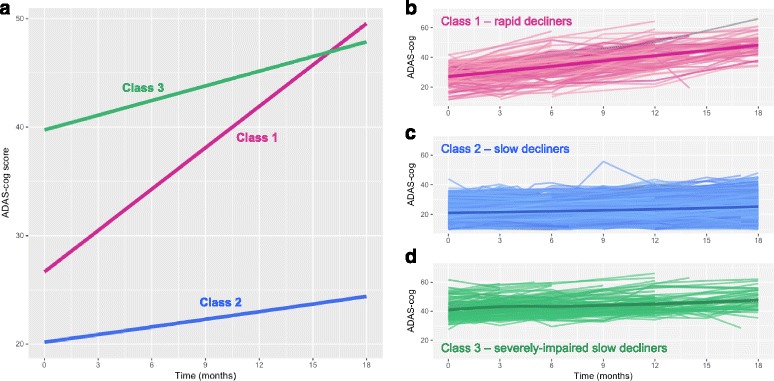
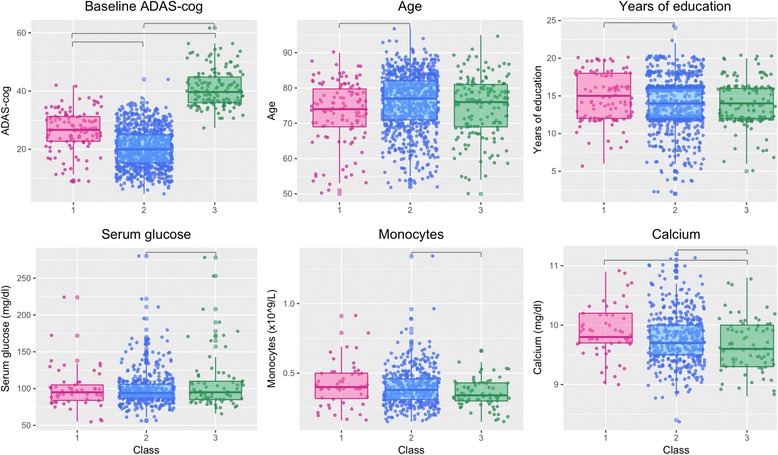
The LCMM resulted in three distinct subgroups of patients, with 10.3% in Class 1, 76.5% in Class 2 and 13.2% in Class 3. While all classes demonstrated some degree of cognitive decline, each demonstrated a different pattern of change in cognitive scores, potentially reflecting different subtypes of AD patients. Class 1 represents rapid decliners with a steep decline in cognition over time, and who tended to be younger and better educated. Class 2 represents slow decliners, while Class 3 represents severely impaired slow decliners: patients with a similar rate of decline to Class 2 but with worse baseline cognitive scores. Class 2 demonstrated a significantly higher proportion of patients with a history of statins use; Class 3 showed lower levels of blood monocytes and serum calcium, and higher blood glucose levels.
Our results, 'learned' from clinical data, indicate the existence of at least three subgroups of Alzheimer's patients, each demonstrating a different trajectory of disease progression. This hypothesis-generating approach has detected distinct AD subgroups that may prove to be discrete endophenotypes linked to specific aetiologies. These findings could enable stratification within a clinical trial or study context, which may help identify new targets for intervention and guide better care.
鉴于阿尔茨海默病(AD)的复杂和渐进性质,需要采用精准医学方法进行诊断和治疗,这就要求确定具有不同生物学和可操作表型定义的患者亚组。
从综合临床试验数据集提取了 1160 名接受安慰剂或未接受治疗且随访时间长达 18 个月的 AD 患者的纵向患者水平数据。我们使用潜在类别混合模型(LCMM)来识别在疾病严重程度(根据阿尔茨海默病评估量表认知子量表评分衡量)随时间变化方面表现出不同变化模式的患者亚组。通过具有最低贝叶斯信息准则的模型选择最佳亚组(类别)数量。使用其他患者水平变量来定义这些亚组的特征,并研究患者特征与疾病进展模式之间的相互作用。
LCMM 产生了三个不同的患者亚组,第 1 类占 10.3%,第 2 类占 76.5%,第 3 类占 13.2%。虽然所有类别都表现出一定程度的认知下降,但每个类别在认知评分的变化模式上都表现出不同,这可能反映了不同类型的 AD 患者。第 1 类代表快速下降者,随着时间的推移认知急剧下降,且往往年龄较小,教育程度较高。第 2 类代表缓慢下降者,第 3 类代表严重受损的缓慢下降者:与第 2 类患者具有相似的下降速度,但基线认知评分较差。第 2 类表现出更高比例的他汀类药物使用史患者;第 3 类显示出较低水平的血液单核细胞和血清钙,以及较高的血糖水平。
我们从临床数据中“学习”的结果表明,至少存在三个 AD 患者亚组,每个亚组都表现出不同的疾病进展轨迹。这种产生假设的方法检测到了不同的 AD 亚组,这些亚组可能被证明是与特定病因相关的离散内表型。这些发现可以在临床试验或研究背景下进行分层,这可能有助于确定新的干预靶点,并指导更好的护理。