Department of Infectious Disease Epidemiology and Modelling, Norwegian Institute of Public Health, Oslo, Norway.
Department of Health Management and Health Economics, University of Oslo, Oslo, Norway.
Pharmacoeconomics. 2018 May;36(5):591-601. doi: 10.1007/s40273-017-0604-3.
New direct-acting antiviral (DAA) drugs have revolutionized the treatment of hepatitis C in recent years.
Our objective was to analyse the cost effectiveness of combinations of different DAAs compared with ribavirin and peginterferon-α-2a, taking into account rebates from tender negotiations.
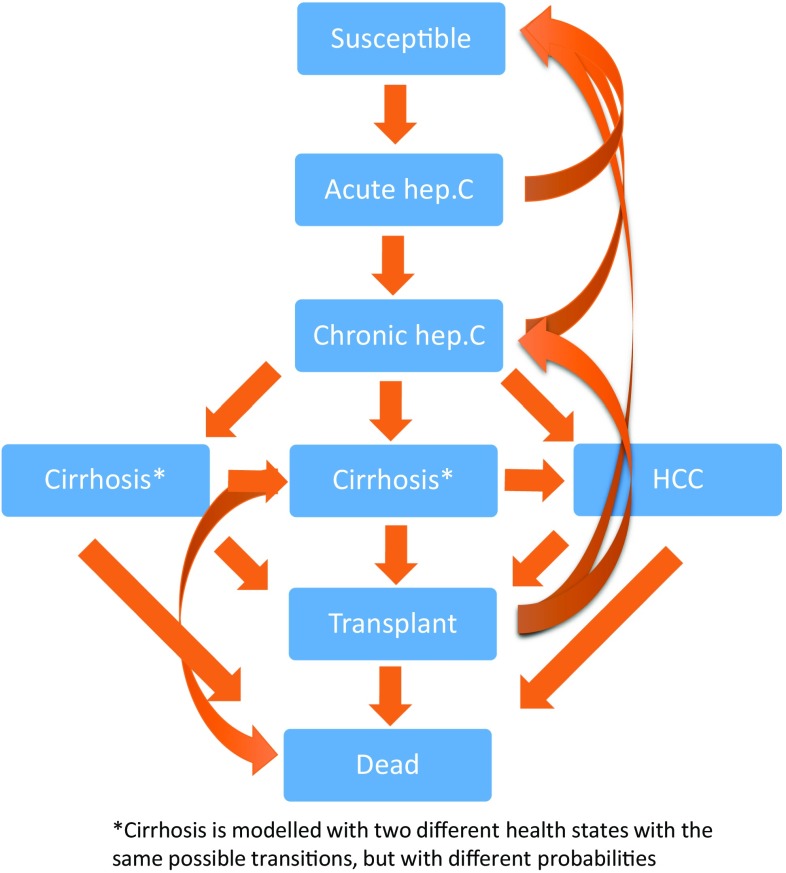
We used a compartmental model specifically developed for Norway to simulate hepatitis C and complications with and without different DAAs. All costs were based on Norwegian fees and estimates, estimating healthcare sector costs for the year 2016. We performed Monte Carlo simulations on uncertain input parameters to facilitate probabilistic sensitivity analyses.
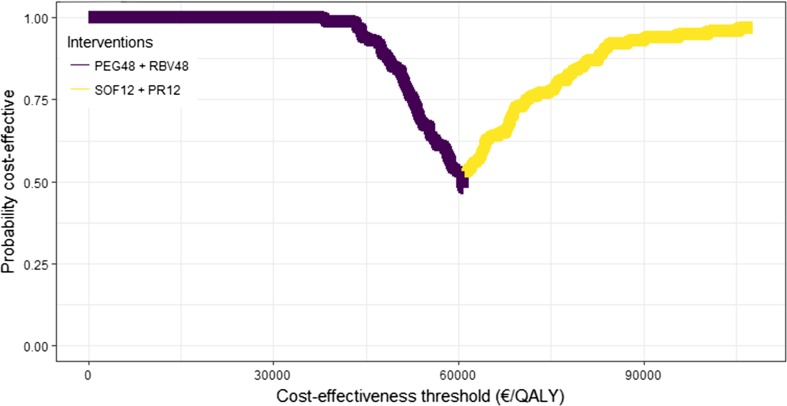
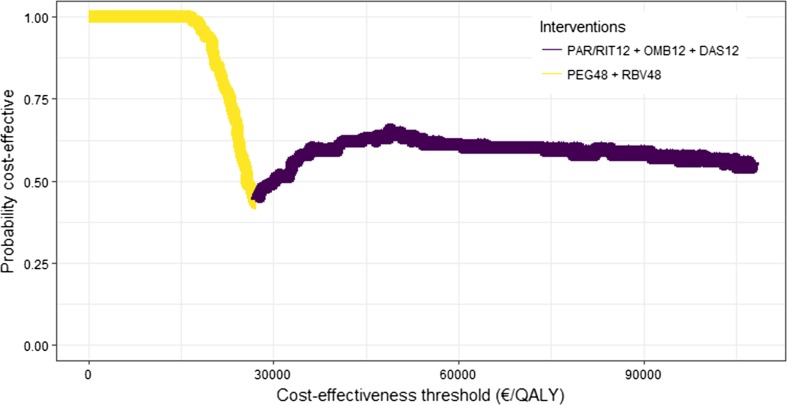
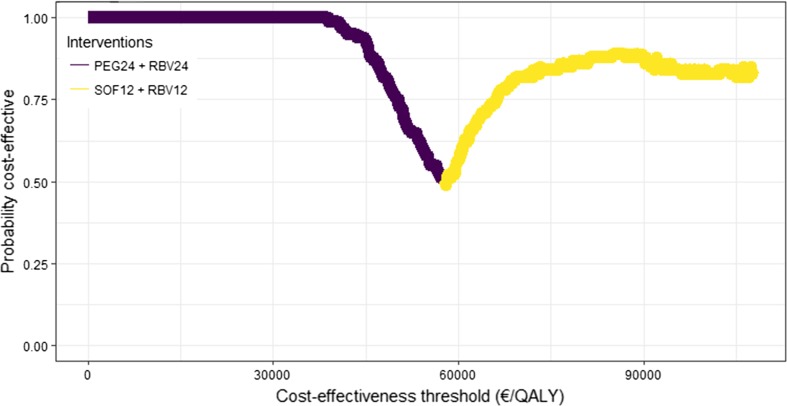
For patients diagnosed with genotype 1, the combination of paritaprevir, ritonavir, ombitasvir and dasabuvir was cost effective compared with eight other available alternatives, given a cost-effectiveness threshold of €70,000 per quality-adjusted life-year. For genotype 2, the combination of sofosbuvir and ribavirin was the most effective and cost-effective alternative for all patients. Among available alternatives for patients with genotype 3, sofosbuvir in combination with peginterferon and ribavirin was the most cost-effective alternative, although the combination of daclatasvir and sofosbuvir was somewhat more effective.
For each of the hepatitis C genotypes 1, 2 and 3, there were combinations of DAAs that were cost effective in a Norwegian setting. As a result of recent tender negotiations in Norway, treating all diagnosed patients with hepatitis C with the most cost-effective DAAs will result in lower total expenditure on these medications compared with 2015.
近年来,新型直接作用抗病毒(DAA)药物彻底改变了丙型肝炎的治疗方式。
我们旨在分析不同 DAA 联合方案与利巴韦林和聚乙二醇干扰素-α-2a 相比的成本效果,同时考虑到招标谈判的回扣。
我们使用专门为挪威开发的房室模型来模拟丙型肝炎及其并发症,同时考虑了不同 DAA 的影响。所有成本均基于挪威的费用和估计值,估算了 2016 年医疗保健部门的成本。我们对不确定输入参数进行了蒙特卡罗模拟,以促进概率敏感性分析。
对于基因型 1 的患者,与其他八种可用替代方案相比,帕立瑞韦、利托那韦、奥比他韦和达卡他韦联合方案在成本效果阈值为每质量调整生命年 70,000 欧元的情况下具有成本效果。对于基因型 2 的所有患者,索非布韦联合利巴韦林是最有效和最具成本效果的替代方案。对于基因型 3 的可用替代方案,索非布韦联合聚乙二醇干扰素和利巴韦林是最具成本效果的替代方案,尽管达卡他韦和索非布韦联合方案的效果略好一些。
在挪威,对于丙型肝炎基因型 1、2 和 3 的每一种情况,都有一些 DAA 联合方案具有成本效果。由于挪威最近的招标谈判,用最具成本效果的 DAA 治疗所有确诊的丙型肝炎患者,与 2015 年相比,这些药物的总支出将会降低。