Adelman Max W, McFarland Deborah A, Tsegaye Mulugeta, Aseffa Abraham, Kempker Russell R, Blumberg Henry M
Department of Medicine, Massachusetts General Hospital, Boston, Massachusetts.
Hubert Department of Global Health, Rollins School of Public Health, Emory University, Atlanta, Georgia.
Open Forum Infect Dis. 2017 Dec 23;5(1):ofx269. doi: 10.1093/ofid/ofx269. eCollection 2018 Jan.
The World Health Organization (WHO) recommends active tuberculosis (TB) case finding and a rapid molecular diagnostic test (Xpert MTB/RIF) to detect TB among people living with HIV (PLHIV) in high-burden settings. Information on the cost-effectiveness of these recommended strategies is crucial for their implementation.
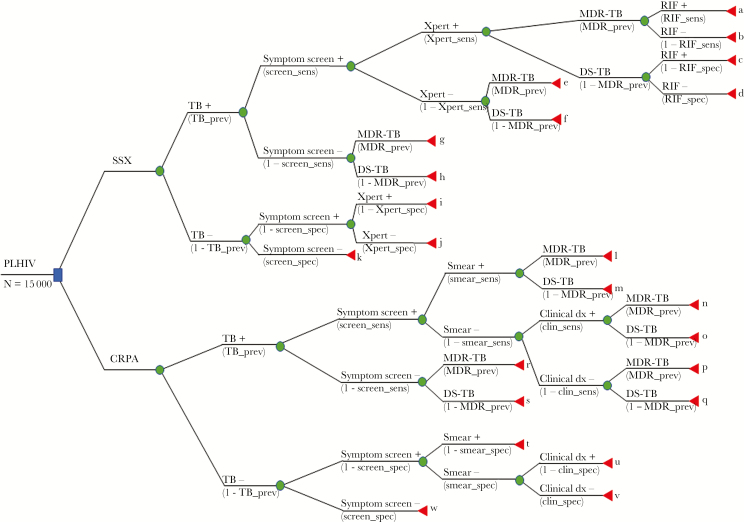
We conducted a model-based cost-effectiveness analysis comparing 2 algorithms for TB screening and diagnosis at Ethiopian HIV clinics: (1) WHO-recommended symptom screen combined with Xpert for PLHIV with a positive symptom screen and (2) current recommended practice algorithm (CRPA; based on symptom screening, smear microscopy, and clinical TB diagnosis). Our primary outcome was US$ per disability-adjusted life-year (DALY) averted. Secondary outcomes were additional true-positive diagnoses, and false-negative and false-positive diagnoses averted.
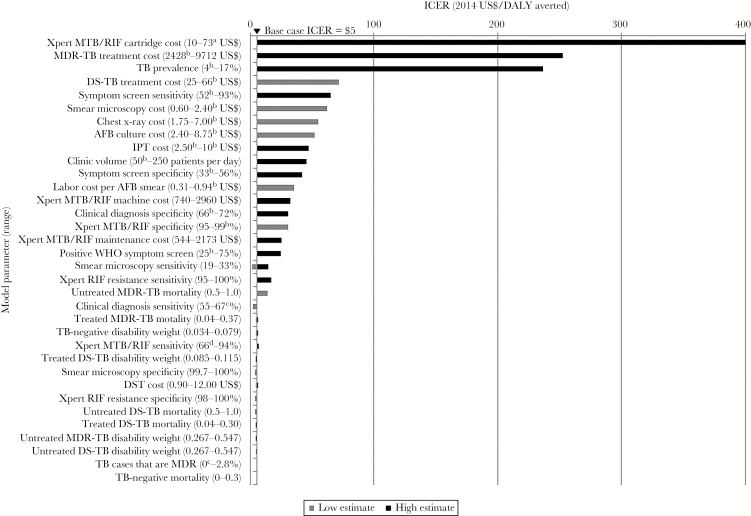
Compared with CRPA, combining a WHO-recommended symptom screen with Xpert was highly cost-effective (incremental cost of $5 per DALY averted). Among a cohort of 15 000 PLHIV with a TB prevalence of 6% (900 TB cases), this algorithm detected 8 more true-positive cases than CRPA, and averted 2045 false-positive and 8 false-negative diagnoses compared with CRPA. The WHO-recommended algorithm was marginally costlier ($240 000) than CRPA ($239 000). In sensitivity analysis, the symptom screen/Xpert algorithm was dominated at low Xpert sensitivity (66%).
In this model-based analysis, combining a WHO-recommended symptom screen with Xpert for TB diagnosis among PLHIV was highly cost-effective ($5 per DALY averted) and more sensitive than CRPA in a high-burden, resource-limited setting.
世界卫生组织(WHO)建议在高负担环境中对艾滋病毒感染者(PLHIV)进行活动性结核病(TB)病例发现,并采用快速分子诊断检测(Xpert MTB/RIF)来检测结核病。这些推荐策略的成本效益信息对于其实施至关重要。
我们进行了一项基于模型的成本效益分析,比较了埃塞俄比亚艾滋病毒诊所的两种结核病筛查和诊断算法:(1)WHO推荐的症状筛查,结合对症状筛查呈阳性的PLHIV进行Xpert检测;(2)当前推荐的实践算法(CRPA;基于症状筛查、涂片显微镜检查和临床结核病诊断)。我们的主要结果是每避免一个伤残调整生命年(DALY)的成本(以美元计)。次要结果是额外的真阳性诊断,以及避免的假阴性和假阳性诊断。
与CRPA相比,将WHO推荐的症状筛查与Xpert相结合具有很高的成本效益(每避免一个DALY的增量成本为5美元)。在一组15000名结核病患病率为6%(900例结核病病例)的PLHIV中,该算法比CRPA多检测出8例真阳性病例,与CRPA相比,避免了2045例假阳性和8例假阴性诊断。WHO推荐的算法比CRPA略贵(240000美元)(239000美元)。在敏感性分析中,症状筛查/Xpert算法在Xpert低敏感性(66%)时占主导地位。
在这项基于模型的分析中,在高负担、资源有限的环境中,将WHO推荐的症状筛查与Xpert相结合用于PLHIV的结核病诊断具有很高的成本效益(每避免一个DALY成本为5美元),并且比CRPA更敏感。