Lee Hee Seung, Chung Moon Jae, Park Jeong Youp, Bang Seungmin, Park Seung Woo, Song Si Young, Chung Jae Bock
Department of Internal Medicine, Institute of Gastroenterology, Yonsei University College of Medicine, Seoul, Korea.
PLoS One. 2018 Feb 5;13(2):e0190835. doi: 10.1371/journal.pone.0190835. eCollection 2018.
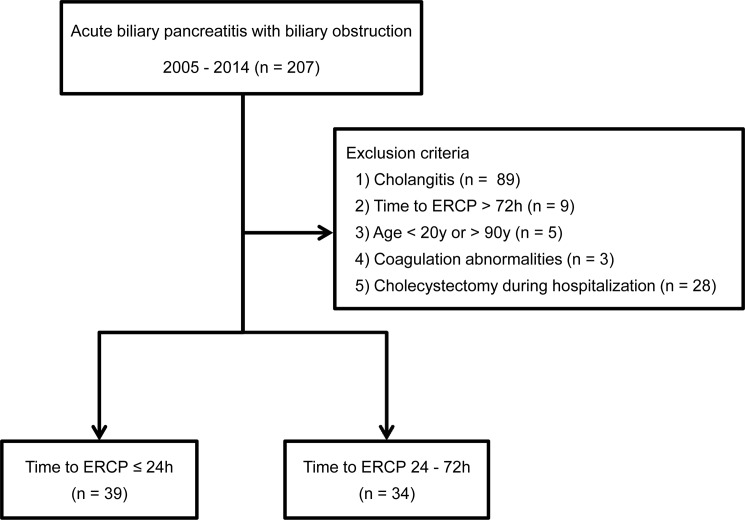
Acute pancreatitis is a common diagnosis worldwide, with gallstone disease being the most prevalent cause (50%). The American College of Gastroenterology recommends urgent endoscopic retrograde cholangiopancreatography (ERCP) (within 24 h) for patients with biliary pancreatitis accompanied by cholangitis. Most international guidelines recommend that ERCP be performed within 72 h in patients with biliary pancreatitis and a bile duct obstruction without cholangitis, but the optimal timing for endoscopy is controversial. We investigated the optimal timing for ERCP in patients with biliary pancreatitis and a bile duct obstruction without cholangitis, and whether performing endoscopy within 24 h is superior to performing it after 24 h. We analyzed the clinical data of 505 patients with newly diagnosed acute pancreatitis, from January 1, 2005 to December 31, 2014. We divided the patients into two groups according to the timing of ERCP: < 24 h (urgent) and 24-72 h (early).Among the 505 patients, 73 were diagnosed with biliary pancreatitis and a bile duct obstruction without cholangitis. The mean age of the patients was 55 years (range: 26-90 years). Bile duct stones and biliary sludge were identified on endoscopy in 45 (61.6%) and 11 (15.0%) patients, respectively. The timing of ERCP within 72 h was not associated with ERCP-related complications (P = 0.113), and the total length of hospital stay was not different between urgent and early ERCP (5.9 vs. 5.7 days, P = 0.174). No significant differences were found in total length of hospitalization or procedural-related complications, in patients with biliary pancreatitis and a bile duct obstruction without cholangitis, according to the timing of ERCP (< 24 h vs. 24-72 h).
急性胰腺炎是全球常见的诊断疾病,胆石症是最常见的病因(50%)。美国胃肠病学会建议,对于伴有胆管炎的胆源性胰腺炎患者,应在24小时内进行紧急内镜逆行胰胆管造影(ERCP)。大多数国际指南建议,对于无胆管炎的胆源性胰腺炎和胆管梗阻患者,应在72小时内进行ERCP,但内镜检查的最佳时机仍存在争议。我们研究了无胆管炎的胆源性胰腺炎和胆管梗阻患者进行ERCP的最佳时机,以及在24小时内进行内镜检查是否优于24小时后进行。我们分析了2005年1月1日至2014年12月31日期间505例新诊断急性胰腺炎患者的临床资料。根据ERCP的时机,将患者分为两组:<24小时(紧急)和24 - 72小时(早期)。在505例患者中,73例被诊断为胆源性胰腺炎和无胆管炎的胆管梗阻。患者的平均年龄为55岁(范围:26 - 90岁)。内镜检查发现45例(61.6%)患者有胆管结石,11例(15.0%)患者有胆泥。72小时内进行ERCP的时机与ERCP相关并发症无关(P = 0.113),紧急ERCP和早期ERCP的住院总时长无差异(5.9天对5.7天,P = 0.174)。对于无胆管炎的胆源性胰腺炎和胆管梗阻患者,根据ERCP的时机(<24小时对24 - 72小时),住院总时长或与操作相关的并发症均无显著差异。