Mantegazza Renato, Antozzi Carlo
Department of Neuroimmunology and Neuromuscular Diseases, Fondazione Istituto Neurologico Carlo Besta, Via Celoria, 11, 20133 Milan, Italy.
Department of Neuroimmunology and Neuromuscular Diseases, Fondazione Istituto Neurologico Carlo Besta, Milan, Italy.
Ther Adv Neurol Disord. 2018 Jan 18;11:1756285617749134. doi: 10.1177/1756285617749134. eCollection 2018.
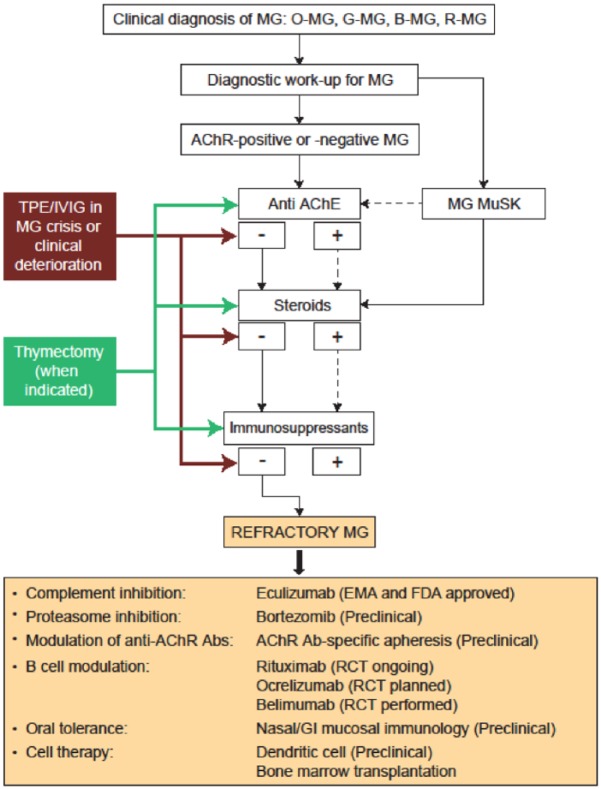
The prognosis for patients with myasthenia gravis (MG) has improved significantly over the past half century, including substantial reductions in mortality and morbidity. However, approximately 10% of patients fails to respond adequately to current therapies and are considered treatment refractory, or treatment intolerant, and up to 80% have disease that fails to achieve complete stable remission. Although patients with autoantibodies to muscle-specific tyrosine kinase (anti-MuSK positive) are more likely to become treatment refractory than those with autoantibodies to the acetylcholine receptor (anti-AChR positive), each of these serotypes is substantially represented in the refractory MG population. Other risk factors for becoming treatment refractory include history of thymoma or thymectomy and female sex. A modified treatment algorithm for MG is proposed: patients who have disease that fails to respond to the stepwise approach to therapy, are treatment intolerant, or who require chronic rescue measures despite ongoing therapy, should be considered treatment refractory and emerging therapies should be considered. Three emerging monoclonal antibody-based therapies are discussed: the anti-B-cell agent rituximab; the terminal complement activation inhibitor eculizumab; and belimumab, which targets B-cell activating factor. Increased understanding of molecular pathophysiology and accurate antibody subtyping in MG should lead to the use of new therapeutic agents and successful management of treatment-refractory patients.
在过去的半个世纪里,重症肌无力(MG)患者的预后有了显著改善,包括死亡率和发病率大幅降低。然而,约10%的患者对当前治疗反应不佳,被认为是治疗难治性或不耐受性的,高达80%的患者疾病未能实现完全稳定缓解。虽然肌肉特异性酪氨酸激酶自身抗体阳性(抗MuSK阳性)的患者比乙酰胆碱受体自身抗体阳性(抗AChR阳性)的患者更易成为治疗难治性患者,但每种血清型在难治性MG患者群体中都占相当比例。成为治疗难治性的其他风险因素包括胸腺瘤或胸腺切除病史以及女性性别。本文提出了一种改良的MG治疗算法:对逐步治疗方法无反应、治疗不耐受或尽管持续治疗仍需长期救援措施的患者,应被视为治疗难治性患者,并应考虑采用新出现的治疗方法。本文讨论了三种基于单克隆抗体的新出现的治疗方法:抗B细胞药物利妥昔单抗;末端补体激活抑制剂依库珠单抗;以及靶向B细胞激活因子的贝利木单抗。对MG分子病理生理学的深入理解和准确的抗体亚型分类应会带来新治疗药物的应用以及难治性患者的成功管理。