Roth Nitzan C, Saberi Behnam, Macklin Jared, Kanel Gary, French Samuel W, Govindarajan Sugantha, Buzzanco Anthony S, Stolz Andrew A, Donovan John A, Kaplowitz Neil
Keck School of Medicine Division of Gastrointestinal and Liver Diseases, University of Southern California Los Angeles CA.
Division of Liver Diseases Icahn School of Medicine at the Mount Sinai Hospital New York NY.
Hepatol Commun. 2017 Dec 4;1(10):1070-1084. doi: 10.1002/hep4.1119. eCollection 2017 Dec.
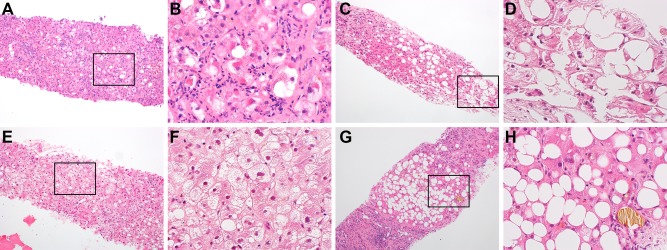
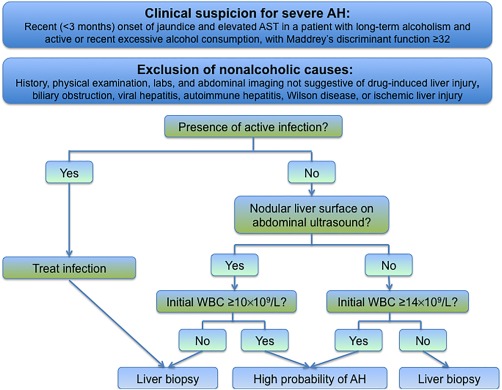
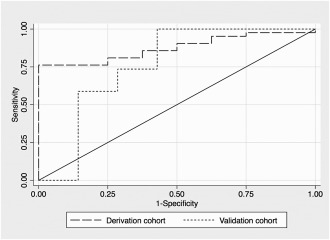
The clinical presentation of alcoholic hepatitis (AH) can be mimicked by other alcoholic liver diseases. The aim of this study was to identify clinical features that predict AH on liver biopsy. Biopsies from patients hospitalized for presumed severe AH were used to identify a derivation cohort (101 patients) and validation cohort (71 patients). Using histologic scores for hepatocyte ballooning, Mallory-Denk bodies, and lobular inflammation, 95 patient biopsies (55%) were classified as definite AH, 55 (32%) as possible AH, and 22 (13%) as no AH. Survival was similar among the groups, but mortality was significantly increased for patients with fatty change ≤50% on initial liver biopsy. An analysis limited to uninfected patients with definite AH or no AH in the derivation cohort identified a greater leukocyte count at admission and radiographic evidence of liver surface nodularity as independent predictors of definite AH on biopsy ( < 0.05). In the derivation cohort, the leukocyte count thresholds for ensuring 100% specificity for diagnosing definite AH were 10 × 10/L if the liver surface was nodular and 14 × 10/L if the liver surface was smooth, with a sensitivity of 76% and an area under the receiver operator characteristic curve of 0.88. In the validation cohort, these thresholds had a specificity of 86%, a sensitivity of 59%, and an area under the receiver operator characteristic curve of 0.72. The combination of an elevated leukocyte count and a nodular liver surface in the absence of active infection retrospectively identified patients with a high likelihood of histologic AH for whom liver biopsy may not be necessary. For patients with suspected severe AH who do not fulfill these criteria, liver biopsy is important to exclude other variants of alcoholic liver disease. ( 2017;1:1070-1084).
酒精性肝炎(AH)的临床表现可能与其他酒精性肝病相似。本研究的目的是确定肝活检时预测AH的临床特征。对因疑似重度AH住院的患者进行活检,以确定一个推导队列(101例患者)和验证队列(71例患者)。使用肝细胞气球样变、马洛里-登克小体和小叶炎症的组织学评分,95例患者的活检标本(55%)被分类为确诊AH,55例(32%)为可能AH,22例(13%)为无AH。各组间生存率相似,但初次肝活检时脂肪变≤50%的患者死亡率显著增加。对推导队列中未感染的确诊AH或无AH患者进行的分析发现,入院时白细胞计数较高以及肝脏表面结节状的影像学证据是活检确诊AH的独立预测因素(P<0.05)。在推导队列中,若肝脏表面呈结节状,诊断确诊AH确保100%特异性的白细胞计数阈值为10×10⁹/L;若肝脏表面光滑,则为14×10⁹/L,敏感性为76%,受试者操作特征曲线下面积为0.88。在验证队列中,这些阈值的特异性为86%,敏感性为59%,受试者操作特征曲线下面积为0.72。白细胞计数升高和肝脏表面结节状且无活动性感染的组合可回顾性地识别出组织学AH可能性高的患者,对这些患者可能无需进行肝活检。对于不符合这些标准的疑似重度AH患者,肝活检对于排除酒精性肝病的其他变异型很重要。(2017;1:1070 - 1084)