Department of Economics, and Oxford Department of International Development, University of Oxford, 3 Mansfield Rd, Oxford OX1 3TB, UK.
Institute for New Economic Thinking, Oxford Martin School, University of Oxford, Eagle House, Walton Well Rd, Oxford OX2 6ED UK.
Health Policy Plan. 2018 Feb 1;33(suppl_1):i14-i23. doi: 10.1093/heapol/czw173.
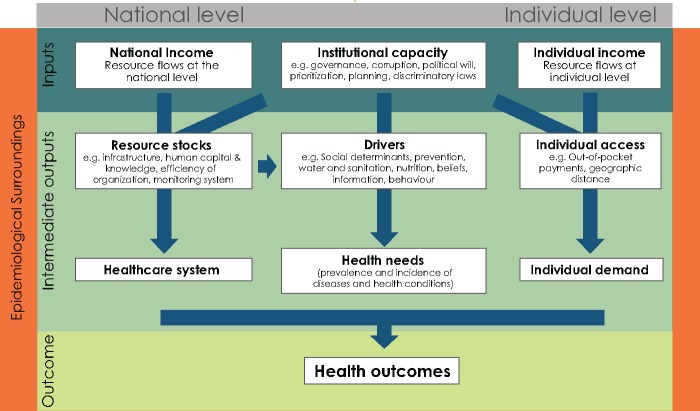
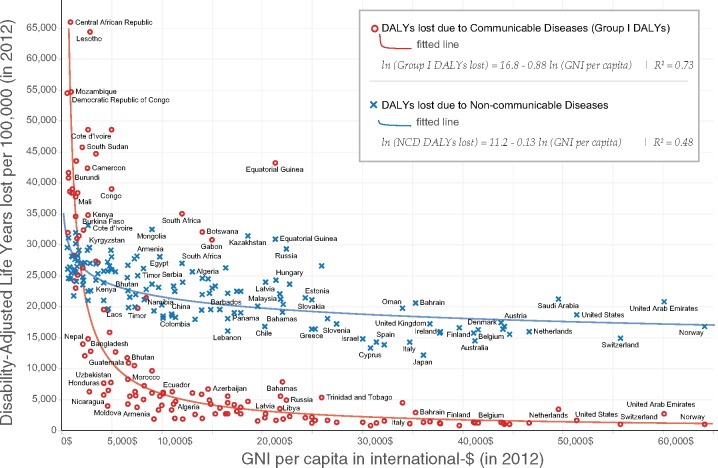
Gross national income (GNI) per capita is widely regarded as a key determinant of health outcomes. Major donors heavily rely on GNI per capita to allocate development assistance for health (DAH). This article questions this paradigm by analysing the determinants of health outcomes using cross-sectional data from 99 countries in 2012. We use disability-adjusted life years (Group I) per capita as our main indicator for health outcomes. We consider four primary variables: GNI per capita, institutional capacity, individual poverty and the epidemiological surroundings. Our empirical strategy has two innovations. First, we construct a health poverty line of 10.89 international-$ per day, which measures the minimum level of income an individual needs to have access to basic healthcare. Second, we take the contagious nature of communicable diseases into account, by estimating the extent to which the population health in neighbouring countries (the epidemiological surroundings) affects health outcomes. We apply a spatial two-stage least-squares model to mitigate the risks of reverse causality. Our model captures 92% of the variation in health outcomes. We emphasize four findings. First, GNI per capita is not a significant predictor of health outcomes once other factors are controlled for. Second, the poverty gap below the 10.89 health poverty line is a good measure of universal access to healthcare, as it explains 19% of deviation in health outcomes. Third, the epidemiological surroundings in which countries are embedded capture as much as 47% of deviation in health outcomes. Finally, institutional capacity explains 10% of deviation in health outcomes. Our empirical findings suggest that allocation frameworks for DAH should not only take into account national income, which remains an important indicator of countries' financial capacity, but also individual poverty, governance and epidemiological surroundings to increase impact on health outcomes.
人均国民总收入(GNI)被广泛认为是健康结果的关键决定因素。主要捐助者严重依赖人均 GNI 来分配用于卫生保健的发展援助(DAH)。本文通过分析 2012 年来自 99 个国家的横截面数据,对这一模式提出质疑。我们使用人均伤残调整生命年(第一组)作为健康结果的主要指标。我们考虑了四个主要变量:人均 GNI、体制能力、个人贫困和流行病学环境。我们的实证策略有两个创新。首先,我们构建了一个 10.89 国际美元/天的健康贫困线,这衡量了个人获得基本医疗保健所需的最低收入水平。其次,我们考虑了传染病的传染性,通过估计邻国(流行病学环境)的人口健康对健康结果的影响程度来衡量。我们采用空间两阶段最小二乘法模型来降低反向因果关系的风险。我们的模型解释了 92%的健康结果的变化。我们强调四个发现。首先,一旦控制了其他因素,人均 GNI 并不是健康结果的显著预测因素。其次,低于 10.89 健康贫困线的贫困差距是衡量全民获得医疗保健的一个很好的指标,因为它解释了健康结果偏差的 19%。第三,各国所处的流行病学环境可以解释健康结果偏差的 47%。最后,体制能力解释了健康结果偏差的 10%。我们的实证结果表明,DAH 的分配框架不仅应考虑国家收入,因为国家收入仍然是国家财政能力的重要指标,还应考虑个人贫困、治理和流行病学环境,以提高对健康结果的影响。