Lancet. 2019 Jun 1;393(10187):2233-2260. doi: 10.1016/S0140-6736(19)30841-4. Epub 2019 Apr 25.
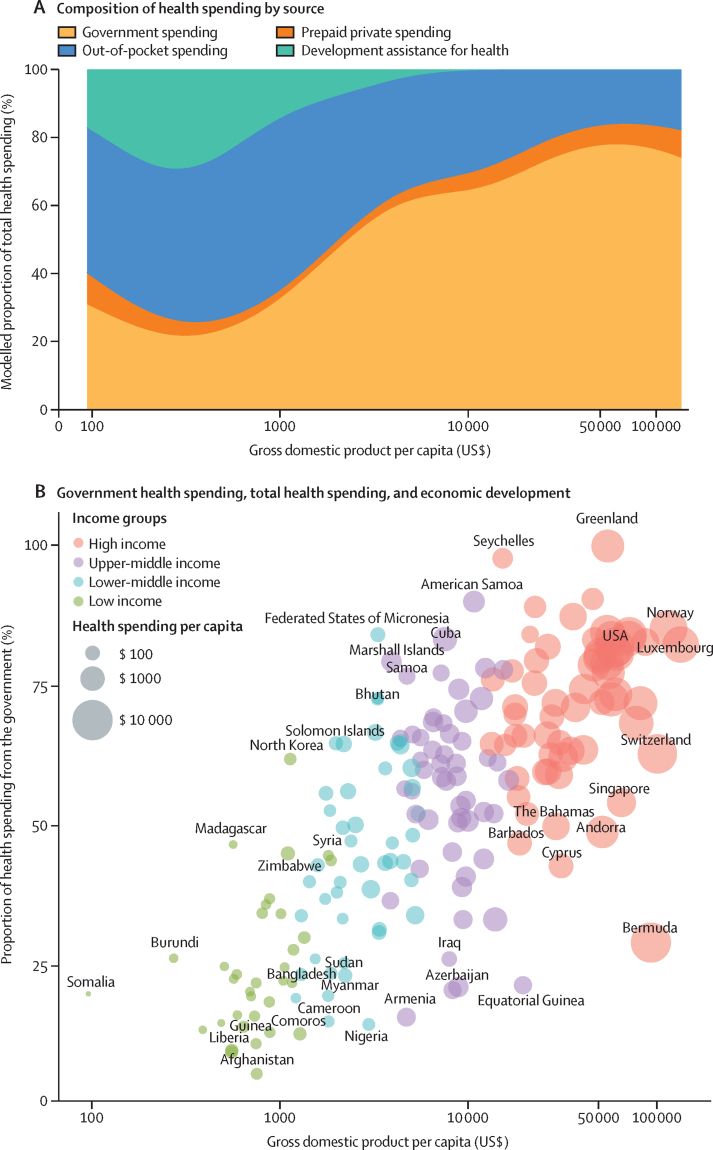
Comprehensive and comparable estimates of health spending in each country are a key input for health policy and planning, and are necessary to support the achievement of national and international health goals. Previous studies have tracked past and projected future health spending until 2040 and shown that, with economic development, countries tend to spend more on health per capita, with a decreasing share of spending from development assistance and out-of-pocket sources. We aimed to characterise the past, present, and predicted future of global health spending, with an emphasis on equity in spending across countries.
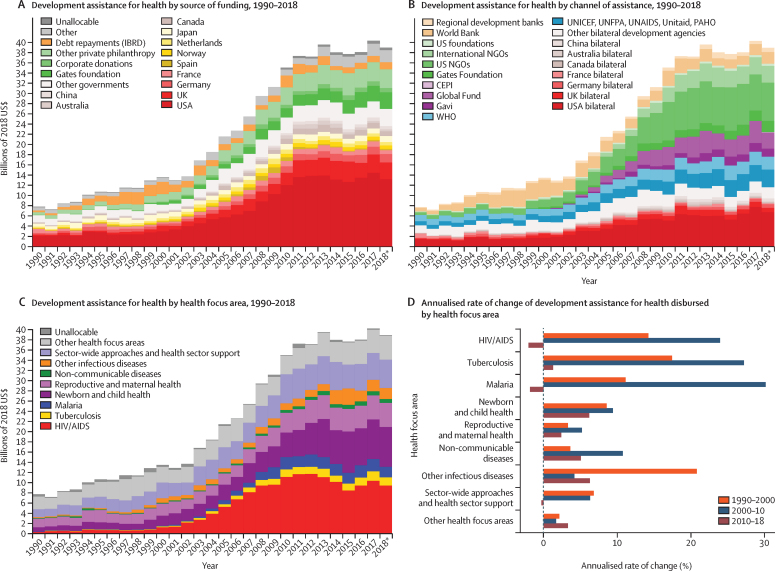
We estimated domestic health spending for 195 countries and territories from 1995 to 2016, split into three categories-government, out-of-pocket, and prepaid private health spending-and estimated development assistance for health (DAH) from 1990 to 2018. We estimated future scenarios of health spending using an ensemble of linear mixed-effects models with time series specifications to project domestic health spending from 2017 through 2050 and DAH from 2019 through 2050. Data were extracted from a broad set of sources tracking health spending and revenue, and were standardised and converted to inflation-adjusted 2018 US dollars. Incomplete or low-quality data were modelled and uncertainty was estimated, leading to a complete data series of total, government, prepaid private, and out-of-pocket health spending, and DAH. Estimates are reported in 2018 US dollars, 2018 purchasing-power parity-adjusted dollars, and as a percentage of gross domestic product. We used demographic decomposition methods to assess a set of factors associated with changes in government health spending between 1995 and 2016 and to examine evidence to support the theory of the health financing transition. We projected two alternative future scenarios based on higher government health spending to assess the potential ability of governments to generate more resources for health.
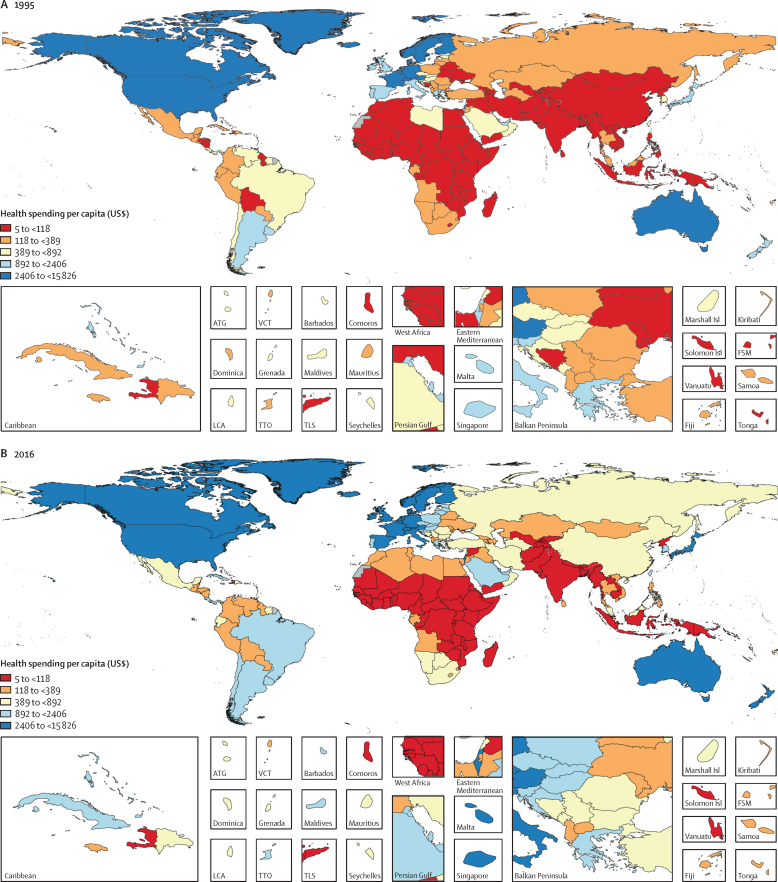
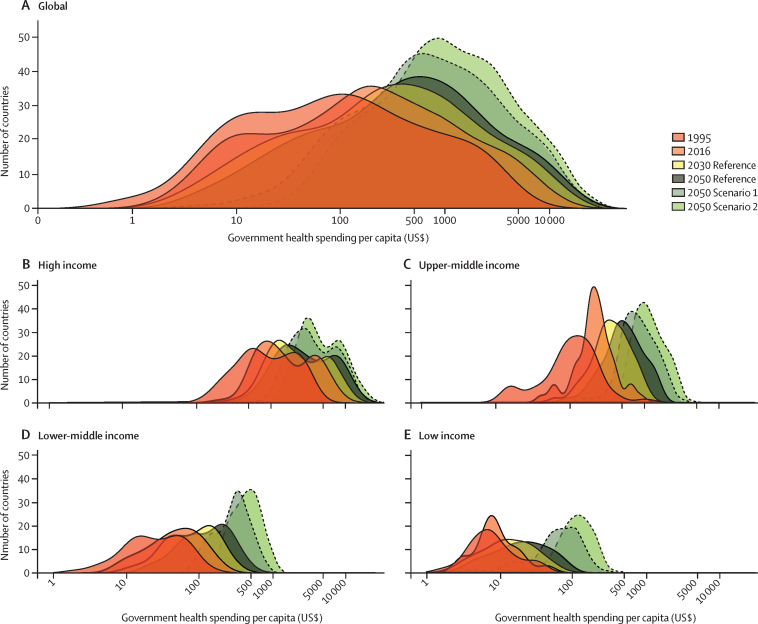
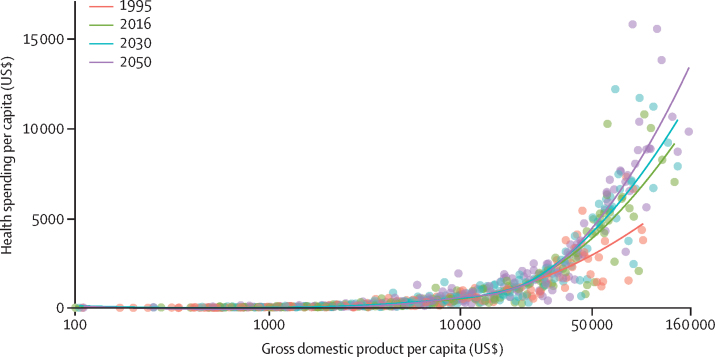
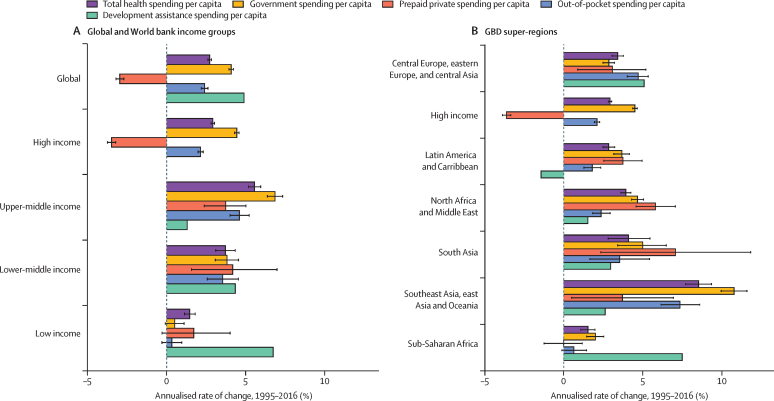
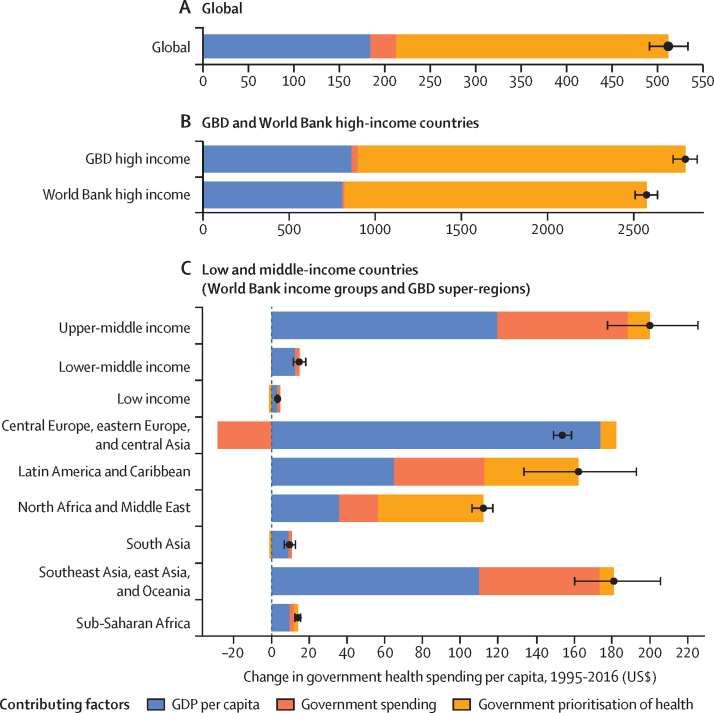
Between 1995 and 2016, health spending grew at a rate of 4·00% (95% uncertainty interval 3·89-4·12) annually, although it grew slower in per capita terms (2·72% [2·61-2·84]) and increased by less than $1 per capita over this period in 22 of 195 countries. The highest annual growth rates in per capita health spending were observed in upper-middle-income countries (5·55% [5·18-5·95]), mainly due to growth in government health spending, and in lower-middle-income countries (3·71% [3·10-4·34]), mainly from DAH. Health spending globally reached $8·0 trillion (7·8-8·1) in 2016 (comprising 8·6% [8·4-8·7] of the global economy and $10·3 trillion [10·1-10·6] in purchasing-power parity-adjusted dollars), with a per capita spending of US$5252 (5184-5319) in high-income countries, $491 (461-524) in upper-middle-income countries, $81 (74-89) in lower-middle-income countries, and $40 (38-43) in low-income countries. In 2016, 0·4% (0·3-0·4) of health spending globally was in low-income countries, despite these countries comprising 10·0% of the global population. In 2018, the largest proportion of DAH targeted HIV/AIDS ($9·5 billion, 24·3% of total DAH), although spending on other infectious diseases (excluding tuberculosis and malaria) grew fastest from 2010 to 2018 (6·27% per year). The leading sources of DAH were the USA and private philanthropy (excluding corporate donations and the Bill & Melinda Gates Foundation). For the first time, we included estimates of China's contribution to DAH ($644·7 million in 2018). Globally, health spending is projected to increase to $15·0 trillion (14·0-16·0) by 2050 (reaching 9·4% [7·6-11·3] of the global economy and $21·3 trillion [19·8-23·1] in purchasing-power parity-adjusted dollars), but at a lower growth rate of 1·84% (1·68-2·02) annually, and with continuing disparities in spending between countries. In 2050, we estimate that 0·6% (0·6-0·7) of health spending will occur in currently low-income countries, despite these countries comprising an estimated 15·7% of the global population by 2050. The ratio between per capita health spending in high-income and low-income countries was 130·2 (122·9-136·9) in 2016 and is projected to remain at similar levels in 2050 (125·9 [113·7-138·1]). The decomposition analysis identified governments' increased prioritisation of the health sector and economic development as the strongest factors associated with increases in government health spending globally. Future government health spending scenarios suggest that, with greater prioritisation of the health sector and increased government spending, health spending per capita could more than double, with greater impacts in countries that currently have the lowest levels of government health spending.
Financing for global health has increased steadily over the past two decades and is projected to continue increasing in the future, although at a slower pace of growth and with persistent disparities in per-capita health spending between countries. Out-of-pocket spending is projected to remain substantial outside of high-income countries. Many low-income countries are expected to remain dependent on development assistance, although with greater government spending, larger investments in health are feasible. In the absence of sustained new investments in health, increasing efficiency in health spending is essential to meet global health targets.
Bill & Melinda Gates Foundation.
全面和可比的各国卫生支出估计数是卫生政策和规划的一个关键投入,也是支持实现国家和国际卫生目标的必要条件。先前的研究跟踪了过去和预测未来的卫生支出,直到 2040 年,并表明,随着经济发展,各国人均卫生支出呈上升趋势,发展援助和自付来源的支出份额减少。我们旨在描述全球卫生支出的过去、现在和未来,重点关注各国之间支出的公平性。
我们从 1995 年到 2016 年估计了 195 个国家和地区的国内卫生支出,分为政府、自付和预付私人卫生支出三类,并从 1990 年到 2018 年估计了发展援助卫生(DAH)。我们使用时间序列规格的线性混合效应模型集合来估计卫生支出的未来情景,以预测 2017 年至 2050 年的国内卫生支出和 2019 年至 2050 年的 DAH。数据来自广泛的卫生支出和收入跟踪来源,经过标准化和转换为 2018 年不变价美元。不完整或低质量的数据进行了建模和不确定性估计,导致了完整的总、政府、预付私人和自付卫生支出以及 DAH 的数据集。报告以 2018 年美元、2018 年购买力平价调整美元以及国内生产总值的百分比表示。我们使用人口分解方法评估了 1995 年至 2016 年政府卫生支出变化的一组因素,并审查了支持卫生融资转型理论的证据。我们根据政府卫生支出增加的情况,提出了两种替代未来情景,以评估政府产生更多卫生资源的潜在能力。
1995 年至 2016 年间,卫生支出以每年 4.00%(95%置信区间为 3.89%-4.12%)的速度增长,尽管按人均计算增长速度较慢(2.72%[2.61%-2.84%]),在 195 个国家中,22 个国家在这一期间的人均卫生支出增加了不到 1 美元。上中等收入国家的人均卫生支出年增长率最高(5.55%[5.18%-5.95%]),主要是由于政府卫生支出的增长,而中下中等收入国家的增长率为 3.71%(3.10%-4.34%),主要来自 DAH。2016 年全球卫生支出达到 8.0 万亿美元(7.8-8.1),占全球经济的 8.6%(8.4%-8.7%),以 2018 年购买力平价调整美元计算为 10.3 万亿美元(10.1-10.6%),高收入国家人均支出 5252 美元(5184-5319),上中等收入国家 491 美元(461-524),中下中等收入国家 81 美元(74-89),低收入国家 40 美元(38-43)。2016 年,全球卫生支出的 0.4%(0.3-0.4)在低收入国家,尽管这些国家占全球人口的 10.0%。2018 年,DAH 的最大比例用于艾滋病毒/艾滋病(95 亿美元,占 DAH 的 24.3%),尽管其他传染病(不包括结核病和疟疾)的支出从 2010 年到 2018 年增长最快(每年 6.27%)。DAH 的主要来源是美国和私人慈善机构(不包括企业捐款和比尔和梅琳达盖茨基金会)。我们首次包括了对中国 DAH 贡献的估计(2018 年 6447 万美元)。全球卫生支出预计将增加到 2050 年的 15.0 万亿美元(14.0-16.0),占全球经济的 9.4%(7.6-11.3%),以 2018 年购买力平价调整美元计算为 21.3 万亿美元(19.8-23.1%),但增长率较低,为每年 1.84%(1.68-2.02%),而且各国之间的支出差距仍在继续。到 2050 年,我们估计在目前的低收入国家中,卫生支出将占 0.6%(0.6-0.7%),尽管到 2050 年,这些国家预计将占全球人口的 15.7%左右。高收入和低收入国家之间的人均卫生支出比率为 130.2(122.9-136.9),预计到 2050 年仍将保持在类似水平(125.9[113.7-138.1])。分解分析确定了政府对卫生部门的日益重视和经济发展是与全球政府卫生支出增长相关的最强因素。未来政府卫生支出情景表明,通过更加重视卫生部门和增加政府支出,人均卫生支出可能增加一倍以上,对目前政府卫生支出水平最低的国家影响更大。
过去二十年来,全球卫生筹资稳步增加,预计未来还会继续增加,尽管增长速度较慢,各国之间的人均卫生支出差距仍然存在。高收入国家以外的自付支出预计仍将保持较大规模。许多低收入国家预计仍将依赖发展援助,尽管随着政府支出的增加,对卫生的更大投资是可行的。在没有持续新的卫生投资的情况下,提高卫生支出效率对于实现全球卫生目标至关重要。
比尔及梅琳达·盖茨基金会。