Singh Preet Mohinder, Borle Anuradha, Kaur Manpreet, Trikha Anjan, Sinha Ashish
Department of Anaesthesia, All India Institute of Medical Sciences, New Delhi, India.
Anesthesiology and Perioperative Medicine, Lewis Katz School of Medicine, Temple University Health System, Philadelphia, USA.
Saudi J Anaesth. 2018 Jan-Mar;12(1):103-111. doi: 10.4103/sja.SJA_382_17.
Thoracic interfascial plane blocks and modification (PECS) have recently gained popularity for analgesic potential during breast surgery. We evaluate/consolidate the evidence on opioid-sparing effect of PECS blocks in comparison with conventional intravenous analgesia (IVA) and paravertebral block (PVB).
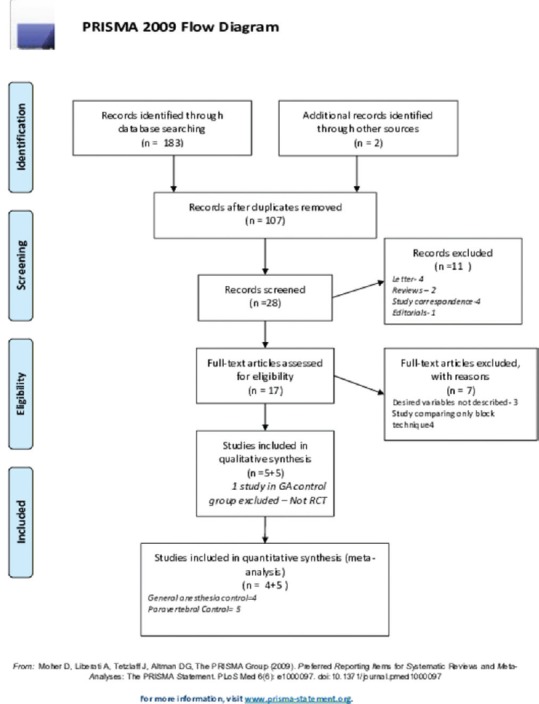
Prospective, randomized controlled trials comparing PECS block to conventional IVA or PVB in patients undergoing breast surgery published till June 2017 were searched in the medical database. Comparisons were made for 24-h postoperative morphine consumption and intraoperative fentanyl-equivalent consumption.
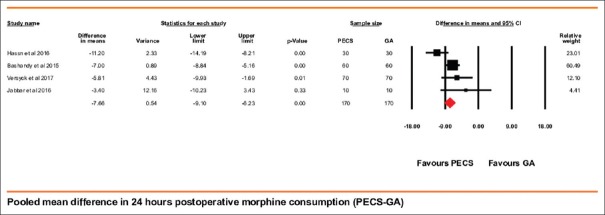
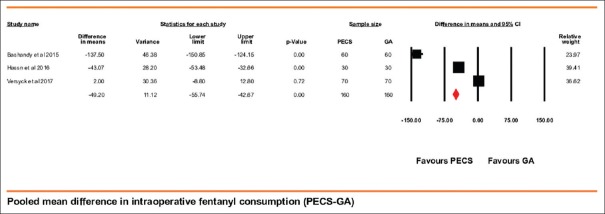
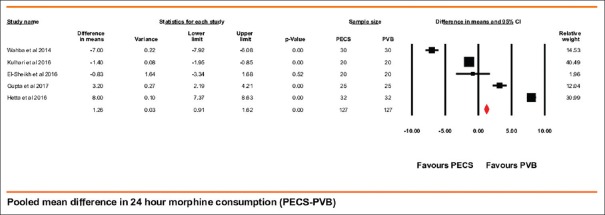
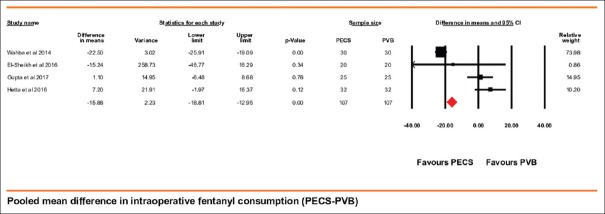
Final analysis included nine trials (PECS vs. IVA 4 trials and PECS vs. PVB 5 trials). PECS block showed a decreased intraoperative fentanyl consumption over IVA by 49.20 mcg (95% confidence interval [CI] =42.67-55.74) ( = 98.47%, < 0.001) and PVB by 15.88 mcg (95% CI = 12.95-18.81) ( = 95.51%, < 0.001). Postoperative, 24-h morphine consumption with PECS block was lower than IVA by 7.66 mg (95% CI being 6.23-9.10) ( = 63.15, < 0.001) but was higher than PVB group by 1.26 mg (95% CI being 0.91-1.62) ( = 99.53%, < 0.001). Two cases of pneumothorax were reported with PVB, and no complication was reported in any other group.
Use of PECS block and its modifications with general anesthesia for breast surgery has significant opioid-sparing effect intraoperatively and during the first 24 h after surgery. It also has higher intraoperative opioid-sparing effect when compared to PVB. During the 1 postoperative day, PVB has slightly more morphine sparing potential that may however be associated with higher complication rates. The present PECS block techniques show marked interstudy variations and need standardization.
胸段筋膜平面阻滞及其改良术(胸肌旁阻滞,PECS)近来因在乳腺手术中的镇痛潜力而受到关注。我们评估并整合了与传统静脉镇痛(IVA)及椎旁阻滞(PVB)相比,PECS阻滞的阿片类药物节省效应的相关证据。
在医学数据库中检索截至2017年6月发表的、比较PECS阻滞与传统IVA或PVB用于乳腺手术患者的前瞻性随机对照试验。对术后24小时吗啡用量及术中芬太尼等效用量进行比较。
最终分析纳入9项试验(PECS与IVA比较4项试验,PECS与PVB比较5项试验)。PECS阻滞组术中芬太尼用量比IVA组减少49.20微克(95%置信区间[CI]=42.67 - 55.74)(P=98.47%,P<0.001),比PVB组减少15.88微克(95% CI = 12.95 - 18.81)(P=95.51%,P<0.001)。术后,PECS阻滞组24小时吗啡用量比IVA组低7.66毫克(95% CI为6.23 - 9.10)(P=63.15,P<0.001),但比PVB组高1.26毫克(95% CI为0.91 - 1.62)(P=99.53%,P<0.001)。PVB组报告了2例气胸,其他组未报告任何并发症。
PECS阻滞及其改良术联合全身麻醉用于乳腺手术,在术中及术后24小时具有显著的阿片类药物节省效应。与PVB相比,其术中阿片类药物节省效应更高。术后第1天,PVB的吗啡节省潜力略大,但可能与更高的并发症发生率相关。目前的PECS阻滞技术在不同研究间存在显著差异,需要标准化。