Perinatology Research Branch, Eunice Kennedy Shriver National Institute of Child Health and Human Development/National Institutes of Health/US Department of Health and Human Services, Bethesda, MD, and Detroit, MI; Department of Obstetrics and Gynecology, Wayne State University School of Medicine, Detroit, MI; Department of Computer Science, Wayne State University College of Engineering, Detroit, MI.
Perinatology Research Branch, Eunice Kennedy Shriver National Institute of Child Health and Human Development/National Institutes of Health/US Department of Health and Human Services, Bethesda, MD, and Detroit, MI; Department of Obstetrics and Gynecology, University of Michigan, Ann Arbor, MI; Department of Epidemiology and Biostatistics, Michigan State University, East Lansing, MI; Center for Molecular Medicine and Genetics, Wayne State University, Detroit, MI.
Am J Obstet Gynecol. 2018 Feb;218(2S):S679-S691.e4. doi: 10.1016/j.ajog.2017.12.229.
The assessment of fetal growth disorders requires a standard. Current nomograms for the assessment of fetal growth in African American women have been derived either from neonatal (rather than fetal) biometry data or have not been customized for maternal ethnicity, weight, height, and parity and fetal sex.
We sought to (1) develop a new customized fetal growth standard for African American mothers; and (2) compare such a standard to 3 existing standards for the classification of fetuses as small (SGA) or large (LGA) for gestational age.
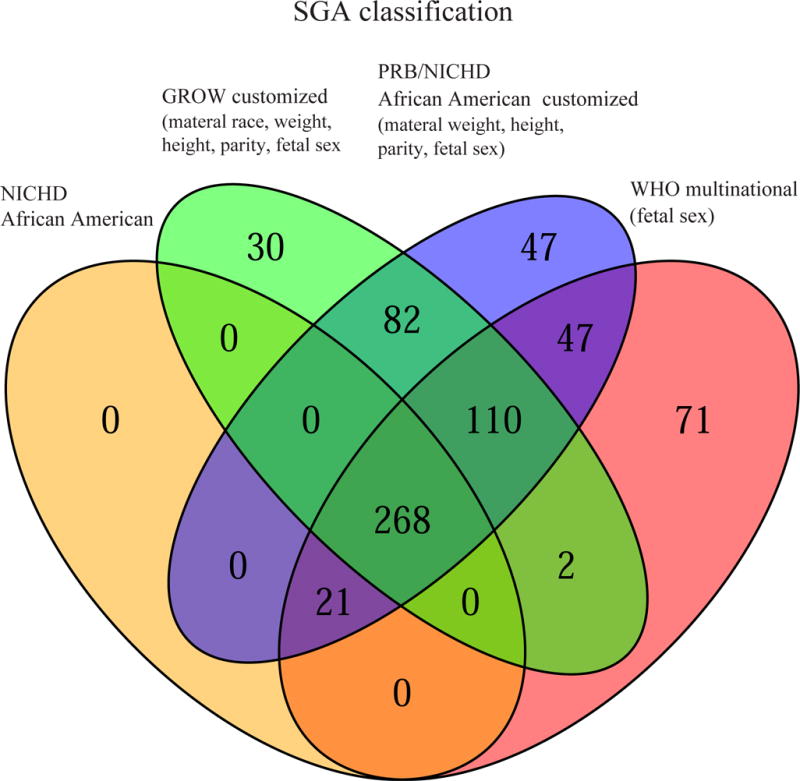
A retrospective cohort study included 4183 women (4001 African American and 182 Caucasian) from the Detroit metropolitan area who underwent ultrasound examinations between 14-40 weeks of gestation (the median number of scans per pregnancy was 5, interquartile range 3-7) and for whom relevant covariate data were available. Longitudinal quantile regression was used to build models defining the "normal" estimated fetal weight (EFW) centiles for gestational age in African American women, adjusted for maternal height, weight, and parity and fetal sex, and excluding pathologic factors with a significant effect on fetal weight. The resulting Perinatology Research Branch/Eunice Kennedy Shriver National Institute of Child Health and Human Development (hereinafter, PRB/NICHD) growth standard was compared to 3 other existing standards--the customized gestation-related optimal weight (GROW) standard; the Eunice Kennedy Shriver National Institute of Child Health and Human Development (hereinafter, NICHD) African American standard; and the multinational World Health Organization (WHO) standard--utilized to screen fetuses for SGA (<10th centile) or LGA (>90th centile) based on the last available ultrasound examination for each pregnancy.
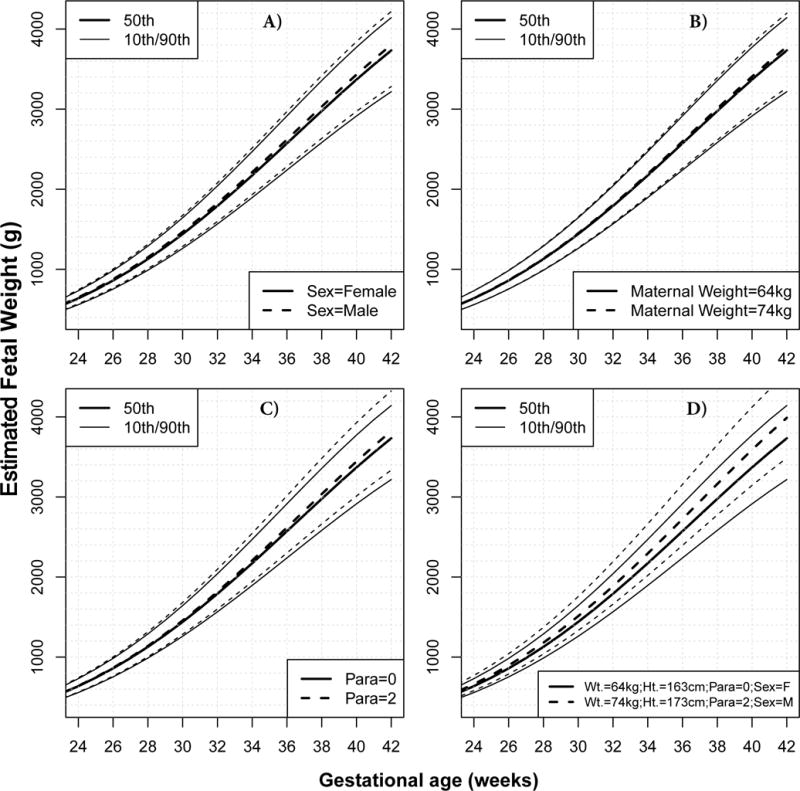
First, the mean birthweight at 40 weeks was 133 g higher for neonates born to Caucasian than to African American mothers and 150 g higher for male than female neonates; maternal weight, height, and parity had a positive effect on birthweight. Second, analysis of longitudinal EFW revealed the following features of fetal growth: (1) all weight centiles were about 2% higher for male than for female fetuses; (2) maternal height had a positive effect on EFW, with larger fetuses being affected more (2% increase in the 95th centile of weight for each 10-cm increase in height); and (3) maternal weight and parity had a positive effect on EFW that increased with gestation and varied among the weight centiles. Third, the screen-positive rate for SGA was 7.2% for the NICHD African American standard, 12.3% for the GROW standard, 13% for the WHO standard customized by fetal sex, and 14.4% for the PRB/NICHD customized standard. For all standards, the screen-positive rate for SGA was at least 2-fold higher among fetuses delivered preterm than at term. Fourth, the screen-positive rate for LGA was 8.7% for the GROW standard, 9.2% for the PRB/NICHD customized standard, 10.8% for the WHO standard customized by fetal sex, and 12.3% for the NICHD African American standard. Finally, the highest overall agreement among standards was between the GROW and PRB/NICHD customized standards (Cohen's interrater agreement, kappa = 0.85).
We developed a novel customized PRB/NICHD fetal growth standard from fetal data in an African American population without assuming proportionality of the effects of covariates, and without assuming that these effects are equal on all centiles of weight; we also provide an easy-to-use centile calculator. This standard classified more fetuses as being at risk for SGA compared to existing standards, especially among fetuses delivered preterm, but classified about the same number of LGA. The comparison among the 4 growth standards also revealed that the most important factor determining agreement among standards is whether they account for the same factors known to affect fetal growth.
评估胎儿生长障碍需要一个标准。目前,评估非裔美国女性胎儿生长的标准要么来自新生儿(而非胎儿)生物测量数据,要么没有针对母亲的种族、体重、身高、产次和胎儿性别进行定制。
我们旨在(1)为非裔美国母亲制定新的定制胎儿生长标准;(2)将这种标准与 3 种现有的用于分类胎儿为小(SGA)或大(LGA)的标准进行比较。
这是一项回顾性队列研究,纳入了来自底特律大都市区的 4183 名女性(4001 名非裔美国人和 182 名白种人),她们在妊娠 14-40 周期间接受了超声检查(每例妊娠的平均扫描次数为 5 次,四分位间距为 3-7 次),并且有相关的协变量数据。采用纵向分位数回归建立模型,定义非裔美国女性胎儿估计体重(EFW)的“正常”胎龄百分位数,调整了母亲的身高、体重和产次以及胎儿性别,并排除对胎儿体重有显著影响的病理因素。由此产生的围产医学研究分支机构/尤尼斯·肯尼迪·施莱佛国立儿童健康与人类发展研究所(以下简称 PRB/NICHD)生长标准与 3 种其他现有标准进行了比较,分别是定制的与妊娠相关的最佳体重(GROW)标准、尤尼斯·肯尼迪·施莱佛国立儿童健康与人类发展研究所(以下简称 NICHD)非裔美国标准和多国世界卫生组织(WHO)标准,这些标准用于根据每个妊娠的最后一次超声检查筛选出 SGA(<第 10 百分位数)或 LGA(>第 90 百分位数)的胎儿。
首先,白种人新生儿的平均出生体重比非裔美国人新生儿高 133 克,男性新生儿比女性新生儿高 150 克;母亲的体重、身高和产次对出生体重有积极影响。其次,对纵向 EFW 的分析揭示了胎儿生长的以下特征:(1)所有体重百分位数对于男性胎儿比女性胎儿高约 2%;(2)母亲的身高对 EFW 有积极影响,身高较高的胎儿影响更大(身高每增加 10 厘米,体重第 95 百分位数增加 2%);(3)母亲的体重和产次对 EFW 有积极影响,这种影响随着妊娠而增加,并且在体重百分位数之间有所不同。第三,NICHD 非裔美国标准的 SGA 筛查阳性率为 7.2%,GROW 标准为 12.3%,WHO 标准为 13%,PRB/NICHD 定制标准为 14.4%。对于所有标准,早产儿的 SGA 筛查阳性率至少是足月儿的 2 倍。第四,GROW 标准的 LGA 筛查阳性率为 8.7%,PRB/NICHD 定制标准为 9.2%,WHO 标准为 10.8%,NICHD 非裔美国标准为 12.3%。最后,标准之间的总体一致性最高是 GROW 和 PRB/NICHD 定制标准(Cohen 评分,kappa=0.85)。
我们从非裔美国人群的胎儿数据中制定了一种新的、独特的 PRB/NICHD 胎儿生长标准,该标准没有假设协变量的影响是成比例的,也没有假设这些影响在所有体重百分位数上是相等的;我们还提供了一个易于使用的百分位数计算器。与现有的标准相比,这种标准将更多的胎儿归类为 SGA 风险较高的胎儿,尤其是早产儿,但将相同数量的 LGA 归类为风险较高的胎儿。对 4 种生长标准的比较还表明,决定标准之间一致性的最重要因素是它们是否考虑了已知影响胎儿生长的相同因素。