Iro M A, Sell T, Brown N, Maitland K
Oxford Vaccine Group, Department of Paediatrics and the NIHR Biomedical Research Centre, University of Oxford, Headington, Oxford, OX3 7LE, UK.
Department of Paediatrics, Salisbury District Hospital, Salisbury, SP2 8BJ, UK.
BMC Pediatr. 2018 Feb 9;18(1):44. doi: 10.1186/s12887-018-1006-1.
The World Health Organization (WHO) recommends rapid intravenous rehydration, using fluid volumes of 70-100mls/kg over 3-6 h, with some of the initial volume given rapidly as initial fluid boluses to treat hypovolaemic shock for children with acute gastroenteritis (AGE) and severe dehydration. The evidence supporting the safety and efficacy of rapid versus slower rehydration remains uncertain.
We conducted a systematic review of randomised controlled trials (RCTs) on 11th of May 2017 comparing different rates of intravenous fluid therapy in children with AGE and moderate or severe dehydration, using standard search terms. Two authors independently assessed trial quality and extracted data. Non-RCTs and non-English articles were excluded. The primary endpoint was mortality and secondary endpoints included adverse events (safety) and treatment efficacy.
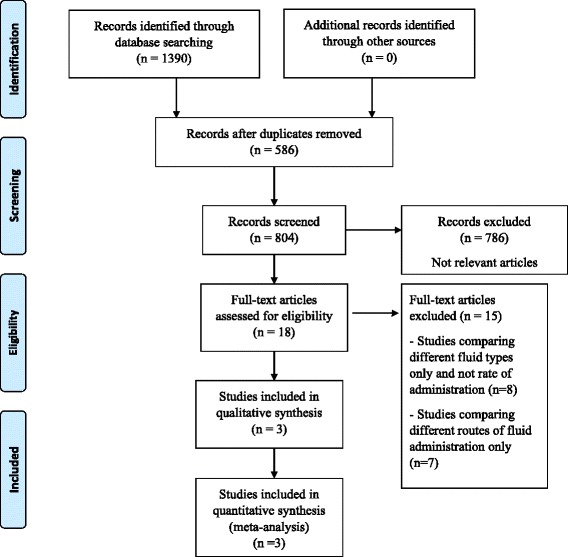
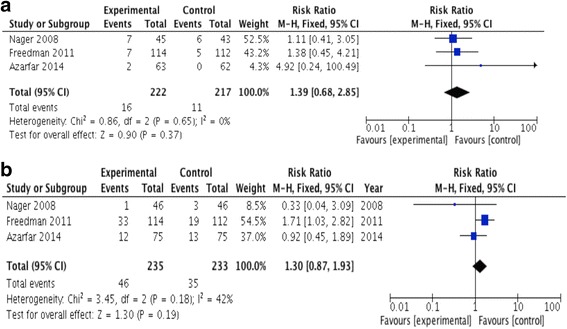
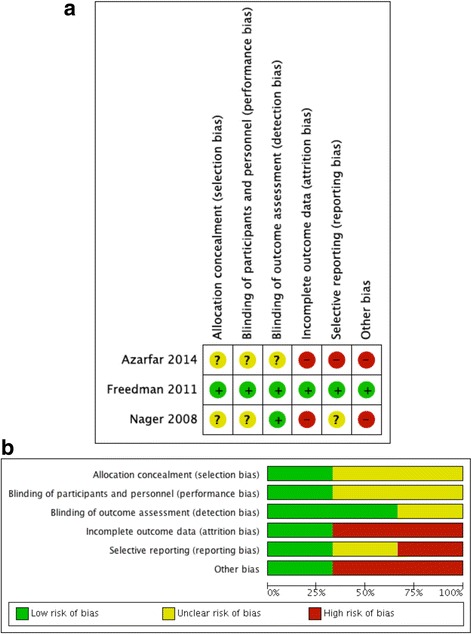
Of the 1390 studies initially identified, 18 were assessed for eligibility. Of these, 3 studies (n = 464) fulfilled a priori criteria for inclusion; most studied children with moderate dehydration and none were conducted in resource-poor settings. Volumes and rates of fluid replacement varied from 20 to 60 ml/kg given over 1-2 h (fast) versus 2-4 h (slow). There was substantial heterogeneity in methodology between the studies with only one adjudicated to be of high quality. There were no deaths in any study. Safety endpoints only identified oedema (n = 6) and dysnatraemia (n = 2). Pooled analysis showed no significant difference between the rapid and slow intravenous rehydration groups for the proportion of treatment failures (N = 468): pooled RR 1.30 (95% CI: 0.87, 1.93) and the readmission rates (N = 439): pooled RR 1.39 (95% CI: 0.68, 2.85).
Despite wide implementation of WHO Plan C guideline for severe AGE, we found no clinical evaluation in resource-limited settings, and only limited evaluation of the rate and volume of rehydration in other parts of the world. Recent concerns over aggressive fluid expansion warrants further research to inform guidelines on rates of intravenous rehydration therapy for severe AGE.
世界卫生组织(WHO)建议采用快速静脉补液法,在3 - 6小时内给予70 - 100毫升/千克的液体量,其中部分初始量作为初始液体推注快速给予,以治疗患有急性肠胃炎(AGE)和严重脱水的儿童的低血容量性休克。支持快速补液与慢速补液的安全性和有效性的证据仍不明确。
2017年5月11日,我们使用标准检索词对比较AGE和中度或重度脱水儿童不同静脉补液治疗速率的随机对照试验(RCT)进行了系统评价。两位作者独立评估试验质量并提取数据。排除非随机对照试验和非英文文章。主要终点是死亡率,次要终点包括不良事件(安全性)和治疗效果。
在最初确定的1390项研究中,有18项被评估是否符合纳入标准。其中,3项研究(n = 464)符合预先设定的纳入标准;大多数研究的是中度脱水儿童,且没有一项在资源匮乏地区进行。补液量和速率方面,1 - 2小时(快速)给予20至60毫升/千克,与2 - 4小时(慢速)给予相对。研究之间在方法上存在很大异质性,只有一项被判定为高质量。任何研究中均无死亡病例。安全性终点仅发现水肿(n = 6)和电解质紊乱(n = 2)。汇总分析显示,快速和慢速静脉补液组在治疗失败比例(N = 468)方面无显著差异:汇总相对危险度为1.30(95%置信区间:0.87,1.93),再入院率(N = 439)方面:汇总相对危险度为1.39(95%置信区间:0.68,2.85)。
尽管WHO针对严重AGE的C计划指南已广泛实施,但我们发现在资源有限的环境中没有临床评估,在世界其他地区对补液速率和量的评估也很有限。近期对积极补液扩容的担忧值得进一步研究,以为严重AGE的静脉补液治疗速率指南提供依据。