Department of Health Services, School of Public Health, University of Washington, Seattle, Washington; Center of Innovation for Veteran-Centered and Value-Driven Care, Veterans Health Administration, Seattle, Washington.
Department of Medicine, University of Iowa Carver College of Medicine, Iowa City, Iowa; Holden Comprehensive Cancer Center, Iowa City, Iowa.
Am J Prev Med. 2018 Apr;54(4):568-575. doi: 10.1016/j.amepre.2018.01.001. Epub 2018 Feb 21.
The purpose of this study is to identify issues faced by Federally Qualified Health Centers (FQHCs) in implementing lung cancer screening in low-resource settings.
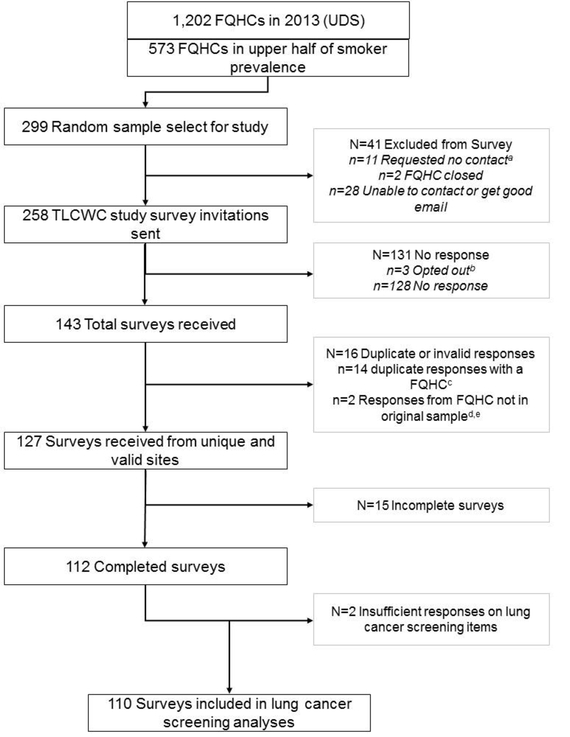
Medical directors of 258 FQHCs serving communities with tobacco use prevalence above the median of all 1,202 FQHCs nationally were sampled to participate in a web-based survey. Data were collected between August and October 2016. Data analysis was completed in June 2017.
There were 112 (43%) FQHC medical directors or surrogates who responded to the 2016 survey. Overall, 41% of respondents were aware of a lung cancer screening program within 30 miles of their system's largest clinic. Although 43% reported that some providers in their system offer screening, it was typically at a very low volume (less than ten/month). Although FQHCs are required to collect tobacco use data, only 13% indicated that these data can identify patients eligible for screening. Many FQHCs reported important patient financial barriers for screening, including lack of insurance (72%), preauthorization requirements (58%), and out-of-pocket cost burdens for follow-up procedures (73%). Only 51% indicated having adequate access to specialty providers to manage abnormal findings, and few reported that leadership had either committed resources to lung cancer screening (12%) or prioritized lung cancer screening (12%).
FQHCs and other safety-net clinics, which predominantly serve low-socioeconomic populations with high proportions of smokers eligible for lung cancer screening, face significant economic and resource challenges to implementing lung cancer screening. Although these vulnerable patients are at increased risk for lung cancer, reducing patient financial burdens and appropriately managing abnormal findings are critical to ensure that offering screening does not inadvertently lead to harm and increase disparities.
本研究旨在确定在资源匮乏环境下实施肺癌筛查时,联邦合格健康中心(FQHC)面临的问题。
抽取全国 1202 家 FQHC 中吸烟率高于中位数的社区的 258 家 FQHC 的医疗主任参与一项基于网络的调查。数据于 2016 年 8 月至 10 月间收集,于 2017 年 6 月完成数据分析。
共有 112 名(43%) FQHC 医疗主任或代理人对 2016 年的调查做出了回应。总体而言,41%的受访者在其系统最大诊所 30 英里范围内了解到一个肺癌筛查项目。尽管 43%的受访者报告其系统中的一些提供者提供筛查服务,但通常数量非常少(每月不到 10 例)。尽管 FQHC 被要求收集烟草使用数据,但只有 13%的人表示这些数据可以识别符合筛查条件的患者。许多 FQHC 报告了筛查的重要患者经济障碍,包括缺乏保险(72%)、预授权要求(58%)以及后续程序的自费负担(73%)。只有 51%的人表示有足够的途径获得专科医生来管理异常发现,很少有人表示领导层已经为肺癌筛查分配资源(12%)或优先考虑肺癌筛查(12%)。
FQHC 和其他医疗保障诊所主要服务于低社会经济阶层、吸烟者比例高、符合肺癌筛查条件的人群,在实施肺癌筛查方面面临着重大的经济和资源挑战。尽管这些弱势群体患者患肺癌的风险增加,但减轻患者的经济负担和适当管理异常发现对于确保提供筛查不会无意中导致伤害和增加差异至关重要。