Kaiser Permanente Center for Health Research, 3800 N Interstate Ave, Portland, OR 97227, USA.
Kaiser Permanente Center for Health Research, 3800 N Interstate Ave, Portland, OR 97227, USA.
Prev Med. 2019 Mar;120:119-125. doi: 10.1016/j.ypmed.2019.01.014. Epub 2019 Jan 24.
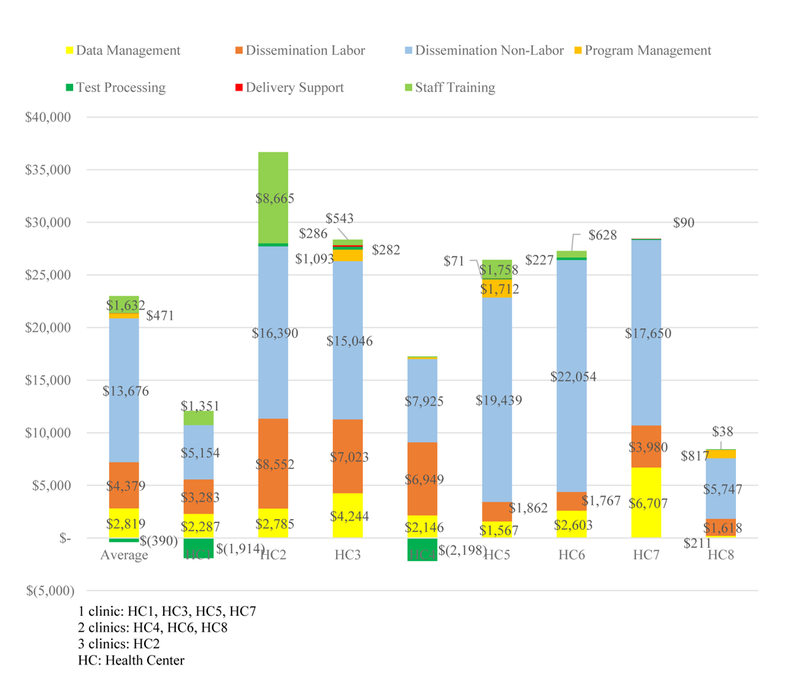
STOP CRC is a cluster-randomized pragmatic study of a colorectal cancer (CRC) screening program within eight federally-qualified health centers (FQHCs) in Oregon and California promoting fecal immunochemical testing (FIT) with appropriate colonoscopy follow-up. Results are presented of a cost-effectiveness analysis of STOP CRC. Organization staff completed activity-based costing spreadsheets, assigning labor hours by intervention activity and job-specific wage rates. Non-labor costs were from study data. Data were collected over February 2014-February 2016; analyses were performed in 2016-2017. Incremental cost-effectiveness ratios (ICERs) using completed FITs adjusted for number of screening-eligible patients (SEPs), as the effectiveness measure were calculated overall and by organization. Intervention delivery costs totaled $305 K across eight organizations (range: $10.2 K-$110 K). Overall delivery cost per SEP was $14.43 (range: $10.37-$19.10). The largest cost category across organizations was implementation, specifically mailing preparation. The overall ICER was $483 per SEP-adjusted completed FIT (range: $96-$1021 among organizations with positive effectiveness). Lagged data accounting for implementation delay produced comparable results. The costs of colonoscopies following abnormal FITs decreased the overall ICER to S409 because usual care clinics generated more such colonoscopies than intervention clinics. Using lagged data, follow-up colonoscopies increase the ICER by 4.3% to $460. Results indicate the complex implications for cost-effectiveness of implementing standard CRC screening within a pragmatic setting involving FQHCs with varied patient populations, clinical structures, and resources. Performance variation across organizations emphasizes the need for future evaluations that inform the introduction of efficient CRC screening to underserved populations.
STOP CRC 是一项在俄勒冈州和加利福尼亚州的 8 家联邦合格健康中心(FQHC)中进行的结直肠癌(CRC)筛查项目的集群随机实用研究,该项目旨在通过适当的结肠镜检查来推广粪便免疫化学检测(FIT)。本文呈现了 STOP CRC 的成本效益分析结果。组织工作人员完成了基于活动的成本核算电子表格,根据干预活动和特定工作的工资率分配劳动时间。非劳动成本来自研究数据。数据收集于 2014 年 2 月至 2016 年 2 月;分析于 2016 年至 2017 年进行。使用经过调整的已完成 FIT 数量作为有效性指标,计算了总体和组织层面的增量成本效益比(ICER)。八项组织的干预措施实施总成本为 305 万美元(范围:10.2 万美元至 110 万美元)。每位符合筛查条件的患者(SEP)的实施成本为 14.43 美元(范围:10.37 美元至 19.10 美元)。组织间最大的成本类别是实施,特别是邮件准备。经过调整的每个 SEP 完成 FIT 的总体 ICER 为 483 美元(范围:组织间的 96 美元至 1021 美元)。考虑实施延迟的滞后数据产生了类似的结果。异常 FIT 后续结肠镜检查的成本降低了总体 ICER 至 409 美元,因为常规护理诊所比干预诊所产生了更多此类结肠镜检查。使用滞后数据,后续结肠镜检查使 ICER 增加了 4.3%,达到 460 美元。结果表明,在涉及具有不同患者群体、临床结构和资源的 FQHC 的实用环境中实施标准 CRC 筛查对成本效益的复杂影响。组织间的绩效差异强调了需要进行未来评估,以便为服务不足的人群引入有效的 CRC 筛查。