School of Economics and Management, Xiamen University of Technology, Xiamen, 361024, China.
Department of Information Management, Yuan Ze University, Taoyuan, 32003, Taiwan.
Int J Equity Health. 2018 Feb 13;17(1):22. doi: 10.1186/s12939-018-0739-7.
Although numerous epidemiological studies on cholecystectomy have been conducted worldwide, only a few have considered the effect of socioeconomic inequalities on cholecystectomy outcomes. Specifically, few studies have focused on the low-income population (LIP).
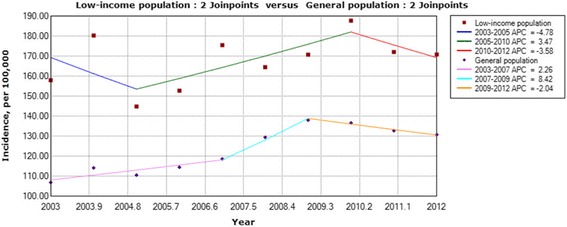
A nationwide prospective study based on the Taiwan National Health Insurance dataset was conducted during 2003-2012. The International Classification of ICD-9-CM procedure codes 51.2 and 51.21-51.24 were identified as the inclusion criteria for cholecystectomy. Temporal trends were analyzed using a joinpoint regression, and the hierarchical linear modeling (HLM) method was used as an analytical strategy to evaluate the group-level and individual-level factors. Interactions between age, gender and SES were also tested in HLM model.
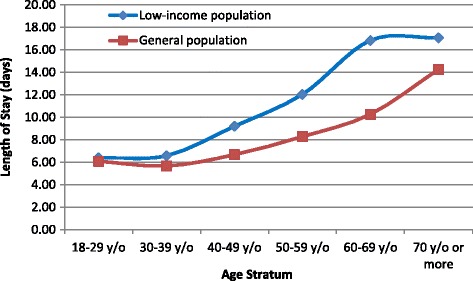
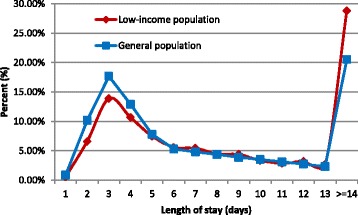
Analyses were conducted on 225,558 patients. The incidence rates were 167.81 (95% CI: 159.78-175.83) per 100,000 individuals per year for the LIP and 123.24 (95% CI: 116.37-130.12) per 100,000 individuals per year for the general population (GP). After cholecystectomy, LIP patients showed higher rates of 30-day mortality, in-hospital complications, and readmission for complications, but a lower rate of routine discharge than GP patients. The hospital costs and length of stay for LIP patients were higher than those for GP patients. The multilevel analysis using HLM revealed that adverse socioeconomic status significantly negatively affects the outcomes of patients undergoing cholecystectomy. Additionally, male sex, advanced age, and high Charlson Comorbidity Index (CCI) scores were associated with higher rates of in-hospital complications and 30-day mortality. We also observed that the 30-day mortality rates for patients who underwent cholecystectomy in regional hospitals and district hospitals were significantly higher than those of patients receiving care in a medical center.
Patients with a disadvantaged finance status appeared to be more vulnerable to cholecystectomy surgery. This result suggested that further interventions in the health care system are necessary to reduce this disparity.
尽管全球范围内已经开展了许多关于胆囊切除术的流行病学研究,但仅有少数研究考虑了社会经济不平等对胆囊切除术结果的影响。具体来说,很少有研究关注低收入人群(LIP)。
本项基于 2003-2012 年台湾全民健康保险数据库的全国性前瞻性研究,将国际疾病分类 ICD-9-CM 操作代码 51.2 和 51.21-51.24 作为纳入标准。采用连接点回归分析时间趋势,使用层次线性建模(HLM)方法作为分析策略,评估群体和个体水平的因素。HLM 模型还测试了年龄、性别和 SES 之间的相互作用。
共分析了 225558 例患者。LIP 的发病率为每 10 万人中每年 167.81(95%CI:159.78-175.83),普通人群(GP)为每 10 万人中每年 123.24(95%CI:116.37-130.12)。胆囊切除术后,LIP 患者的 30 天死亡率、院内并发症和并发症再入院率较高,但常规出院率低于 GP 患者。LIP 患者的住院费用和住院时间均高于 GP 患者。使用 HLM 的多水平分析表明,不利的社会经济地位显著影响接受胆囊切除术患者的结局。此外,男性、高龄和高 Charlson 合并症指数(CCI)评分与较高的院内并发症和 30 天死亡率相关。我们还观察到,在地区医院和区医院接受胆囊切除术的患者的 30 天死亡率明显高于在医疗中心接受治疗的患者。
经济地位处于劣势的患者似乎更容易受到胆囊切除术的影响。这一结果表明,有必要在医疗保健系统中进一步进行干预,以减少这种差异。