Zhang Feng, Zhang Kai, Tian Hai-Jun, Wu Ai-Min, Cheng Xiao-Fei, Zhou Tang-Jun, Zhao Jie
Ninth People's Hospital, Department of Orthopaedics, Shanghai Key Laboratory of Orthopaedic Implants, Shanghai Jiaotong University School of Medicine, 639 Zhizaoju Road, Shanghai, People's Republic of China.
J Orthop Surg Res. 2018 Feb 12;13(1):34. doi: 10.1186/s13018-018-0737-x.
To investigate the distribution and characteristics of the lumbar intervertebral disc height (IDH) in asymptomatic Asian population and to determine whether the lumbar IDH is related to the lumbar spine sagittal alignment.
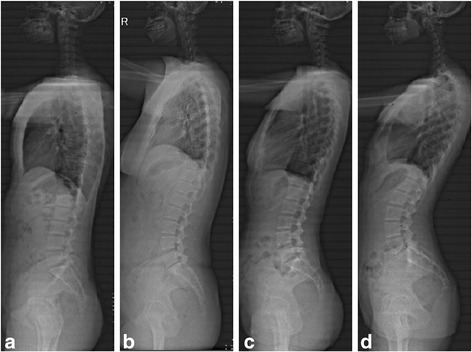
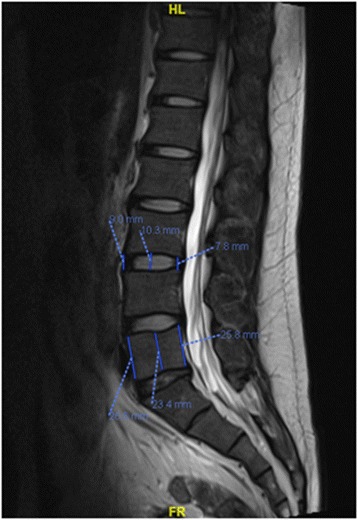
A cohort of 169 cases of asymptomatic volunteers was enrolled from January 2014 to July 2016. All participants underwent magnetic resonance imaging of the lumbar spine and panoramic radiography of the spine. Panoramic radiographs of the spine were taken to evaluate pelvic incidence (PI), sacral slope (SS), and pelvic tilt (PT) using Surgimap® software. Roussouly classification was utilized to categorize all subjects according to the four subtypes of sagittal alignment. The IDH was measured on the MRI mid-saggital section of the vertebral body. The relationships between lumbar IDH and spine-pelvic parameters were also assessed using the Spearman correlation analysis.
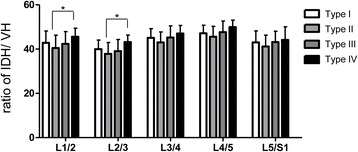
The reference value ranges of IDH in asymptomatic Asian volunteers between L1/2, L2/3, L3/4, L4/5, and L5/S1 were (6.25, 10.99), (6.97, 12.08), (7.42, 13.3), (7.76, 14.57),and (7.11, 13.12) mm, respectively. Based on the above reference value, the high lumbar intervertebral space is defined as more than 14 mm. According to the Roussouly Classification, there are 33 cases in type I, 48 in type II, 66 in type III, and 22 in type IV. According to the definition of the high IDH, there are two cases in type I, three in type II, nine in type III, and eight in type IV. The results indicated that people in the Roussouly III and IV subtypes had greater values for IDH compared to those of Roussouly I and II subtypes, and the spinopelvic parameters were partly correlated with IDH in different subtypes. In addition, levels L4-L5 showed the highest IDH for all four groups followed by the L3-L4 and L5-S1 levels, and the value of L3-L4 is equivalent to that of L5-S1. All type groups showed moderate and positive correlations between the PI and IDH except the level of L1-L2 in type IV.
The IDH may influence the lumbar spine sagittal alignment in asymptomatic Asian adults. Moreover, pre-operative evaluation of IDH is useful for selection of optimal cage size and reconstruction of spinal alignment.
研究无症状亚洲人群腰椎间盘高度(IDH)的分布及特征,并确定腰椎IDH是否与腰椎矢状位对线有关。
2014年1月至2016年7月纳入169例无症状志愿者队列。所有参与者均接受腰椎磁共振成像及脊柱全景X线摄影。使用Surgimap®软件对脊柱全景X线片进行分析,以评估骨盆入射角(PI)、骶骨倾斜角(SS)和骨盆倾斜角(PT)。根据矢状位对线的四种亚型,采用鲁索利分类法对所有受试者进行分类。在椎体的MRI矢状中线上测量IDH。还采用Spearman相关分析评估腰椎IDH与脊柱-骨盆参数之间的关系。
无症状亚洲志愿者L1/2、L2/3、L3/4、L4/5和L5/S1节段IDH的参考值范围分别为(6.25,10.99)、(6.97,12.08)、(7.42,13.3)、(7.76,14.57)和(7.11,13.12)mm。根据上述参考值,将高腰椎间隙定义为大于14mm。根据鲁索利分类,I型33例,II型48例,III型66例,IV型22例。根据高IDH的定义,I型2例,II型3例,III型9例,IV型8例。结果表明,与鲁索利I型和II型亚型相比,鲁索利III型和IV型亚型的IDH值更大,且不同亚型中脊柱-骨盆参数与IDH部分相关。此外,所有四组中L4-L5节段的IDH最高,其次是L3-L4和L5-S1节段,L3-L4节段的值与L5-S1节段相当。除IV型L1-L2节段外,所有类型组的PI与IDH之间均呈中度正相关。
IDH可能影响无症状亚洲成年人的腰椎矢状位对线。此外,术前评估IDH有助于选择最佳椎间融合器尺寸及重建脊柱对线。